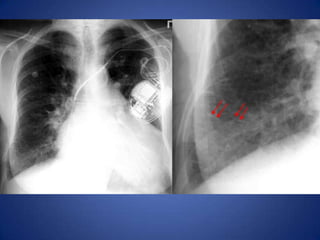
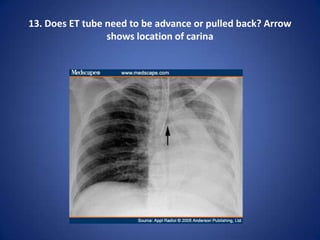
Based on the provided chest x-ray, the ET tube tip is located above the carina and in the proper position within the trachea. It does not appear to need adjustment. Feeding through the R/T tube would be appropriate.
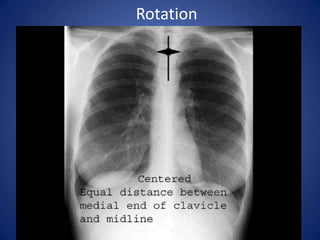
Film QualityPA orAP view.Upright/Erect or SupineBreath : Inspiration or ExpirationX-ray penetration : Under- or Over-Rotation
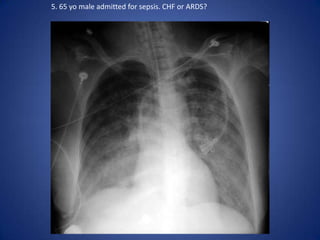
5.
PA vs APviewsPA viewScapula is seen in periphery of thoraxClavicles project over lung fieldsPosterior ribs are distinctPosition of markersAP viewScapulae are over lung fieldsClavicles are above the apex of lung fieldsPosition of markersAnterior ribs are distinct
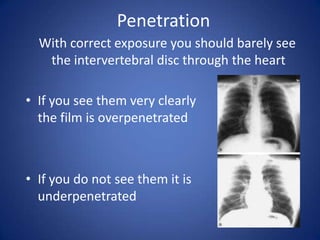
Penetration With correct exposure you should barely see the intervertebral disc through the heartIf you see them very clearly the film is overpenetratedIf you do not see them it is underpenetrated
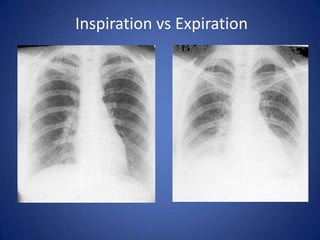
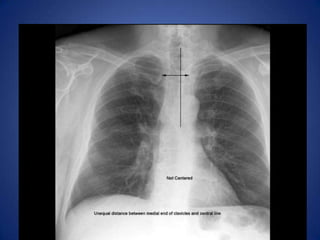
Pitfalls to ChestX-ray InterpretationPoor inspirationOver or under penetrationRotationForgetting the path of the x-ray beam
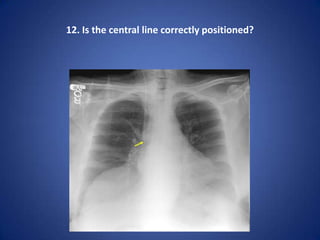
12.
Normal Chest X-rayCardiacStructuresPositionMore central in younger infants and childrenMore on the L side in older infants and teensSizeCARDIO-THORACIC RATIO!Cardiac diameter :normal individuals < 15.5 cm in males; <14.5 cm in females.A change in diameter of greater than 1.5 cm between two X-rays is significant.
13.
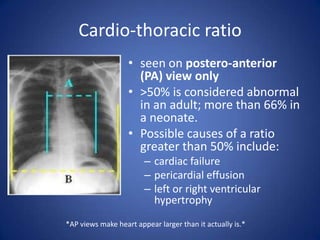
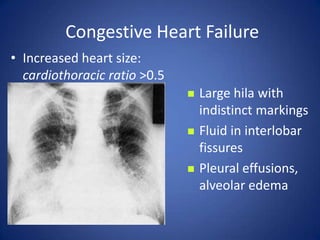
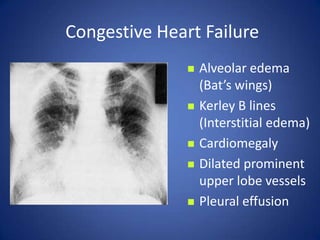
Cardio-thoracic ratioseen onpostero-anterior (PA) view only>50% is considered abnormal in an adult; more than 66% in a neonate.Possible causes of a ratio greater than 50% include:cardiac failurepericardial effusionleft or right ventricular hypertrophy*AP views make heart appear larger than it actually is.*
14.
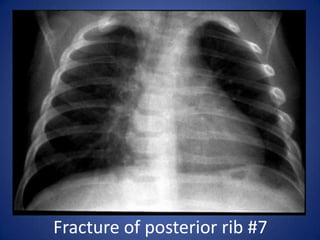
Normal Chest X-ray1.Soft tissue structuresShadows, most commonly, breast2. Bony structuresCount the ribs8 – 10 ribs should be visible on inspirationClavicle placement at 2-3 intercostal space (if not, may be rotated)
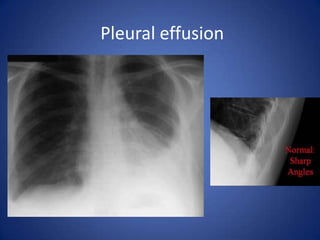
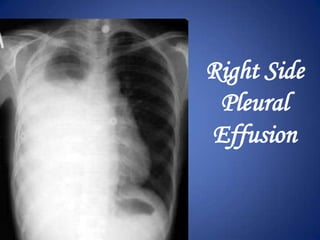
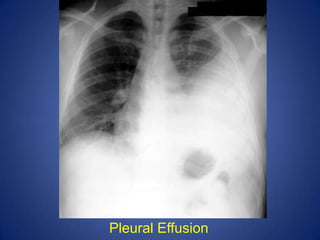
Normal Chest X-ray4. LungsStartat the top and compare the R and LTrachea should be midline over the thoracic vertebrae and air filledLung parenchyma becomes lighter as you go down the lung. If not, it may indicate a lower lobe or pleural effusion
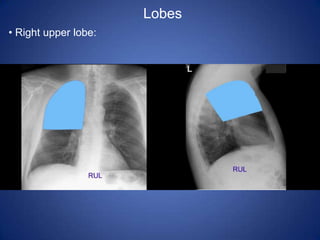
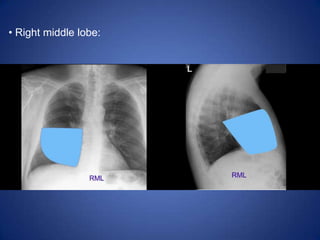
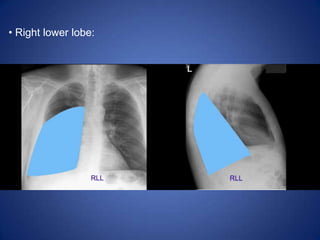
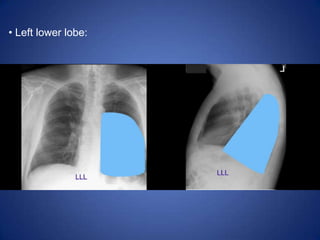
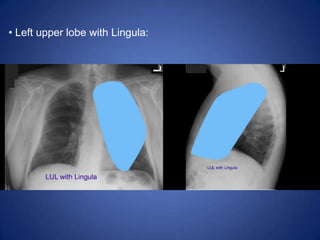
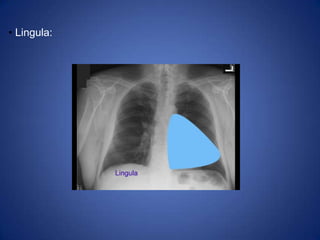
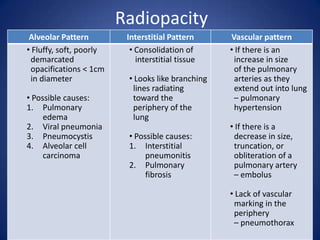
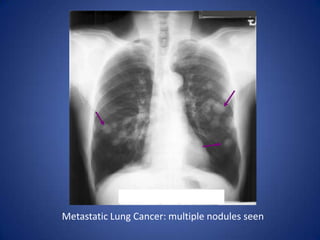
Lobes Right upperlobe: Right middle lobe: Right lower lobe: Left lower lobe: Left upper lobe with Lingula:Lingula: Left upper lobe - upper division:Abnormal Chest X-rayRadiopacity (whiteness) = increased densityRadiotranslucency (blackness) = decreased density
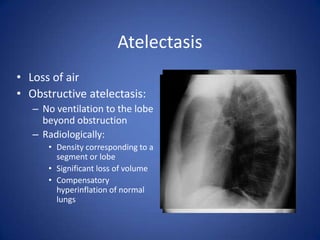
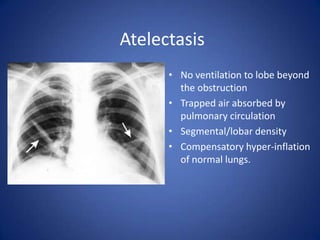
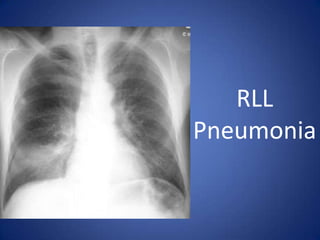
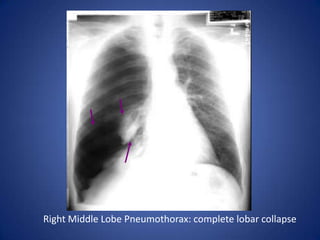
AtelectasisLoss of airObstructiveatelectasis:No ventilation to the lobe beyond obstructionRadiologically:Density corresponding to a segment or lobeSignificant loss of volumeCompensatory hyperinflation of normal lungs
30.
No ventilation tolobe beyond the obstructionTrapped air absorbed by pulmonary circulationSegmental/lobar densityCompensatory hyper-inflation of normal lungs.Atelectasis
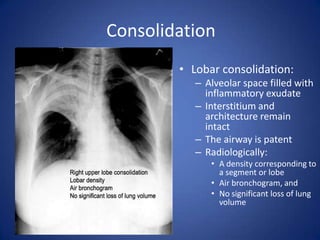
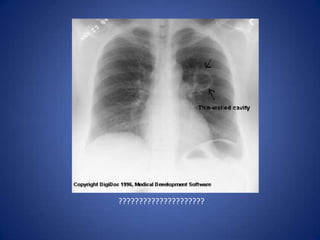
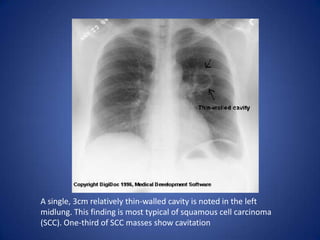
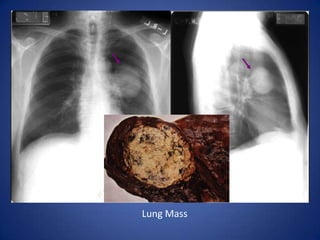
A single, 3cmrelatively thin-walled cavity is noted in the left midlung. This finding is most typical of squamous cell carcinoma (SCC). One-third of SCC masses show cavitation
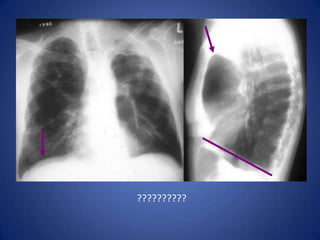
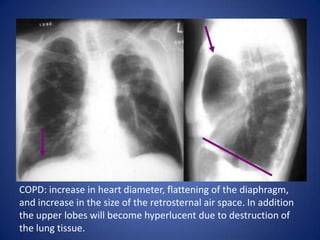
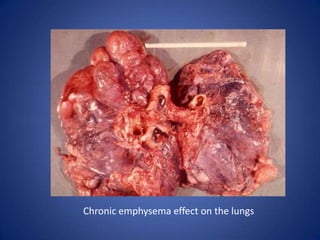
COPD: increase inheart diameter, flattening of the diaphragm, and increase in the size of the retrosternal air space. In addition the upper lobes will become hyperlucent due to destruction of the lung tissue.
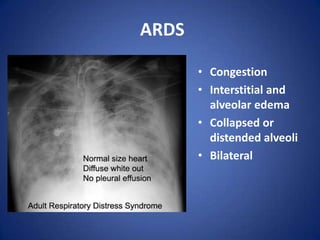
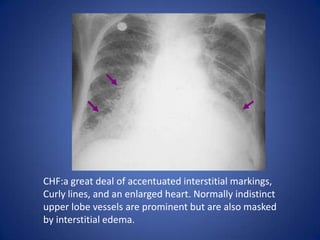
CHF:a great dealof accentuated interstitial markings, Curly lines, and an enlarged heart. Normally indistinct upper lobe vessels are prominent but are also masked by interstitial edema.