Downloaded 1,931 times


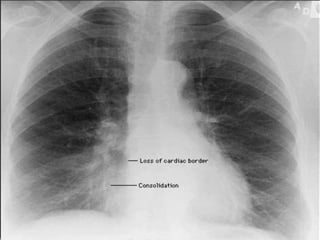













The document outlines various signs observed in chest X-rays, describing their appearances and clinical significance in diagnosing conditions such as fluid presence, consolidation, and lung collapse. Key signs include the silhouette sign, air bronchogram, deep sulcus sign, and golden 'S' sign, each indicating different underlying issues in lung anatomy and pathology. The document serves as a comprehensive reference for radiological anatomy related to thoracic imaging and its implications for patient care.














































































