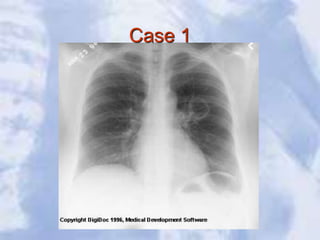
1. The document provides guidance on systematically interpreting a chest x-ray by first examining the bony framework and then soft tissues, lung fields, diaphragm, mediastinum, heart, abdomen and neck.
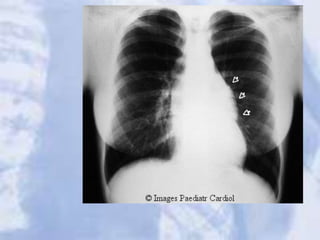
2. Key aspects to evaluate include the lung fields, hila, diaphragm, heart size and location, mediastinal structures, and presence of any masses, infiltrates or abnormalities.
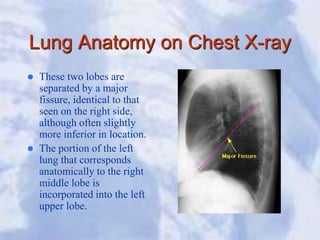
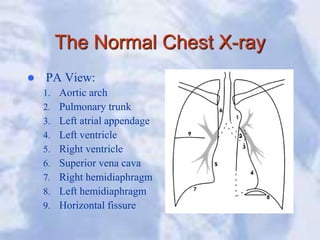
3. Anatomical structures are also described including lung lobes, fissures, and appearances on PA versus lateral views to aid localization of findings.
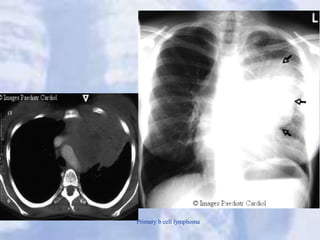
4. Examples of common pathologies are shown such as pneumonia, lung cancer, COPD, and cardiomegaly along with






































































![A widened mediastinum can be indicative of several pathologies
aortic aneurysm]
aortic dissection]
aortic unfolding
. Ruptured Aorta
hilar lymphadenopathy
anthrax inhalation. A widened mediastinum was found in 7 of the first 10 victims
infected by anthrax (Bacillus anthracis) in 2001
esophageal rupture - presents usually with pneumomediastinum and pleural
effusion. It is diagnosed with water soluble swallowed contrast.
mediastinal mass
mediastinitis
cardiac tamponade]
pericardial effusion
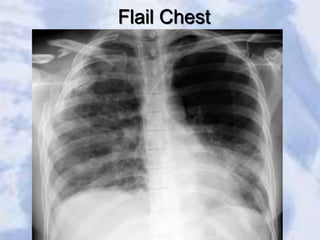
thoracic vertebrae fractures in trauma patients.](https://image.slidesharecdn.com/cxr-230209182351-04a08904/85/cxr-ppt-78-320.jpg)