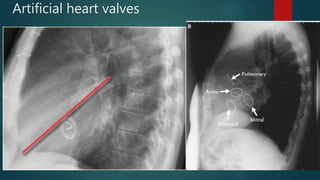
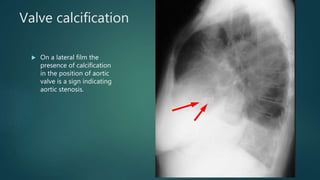
Valvular heart disease affects the mitral, aortic, tricuspid, and pulmonary valves. Imaging plays an important role in assessing valve stenosis and regurgitation, effects on ventricular function, and associated pulmonary pathologies. Echocardiography is the main imaging modality and can evaluate valve structure and function, ventricular size, and pressures. Chest x-ray is also useful and can show valve calcification and chamber enlargement. Imaging is used to assess disease severity and guide management.
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

