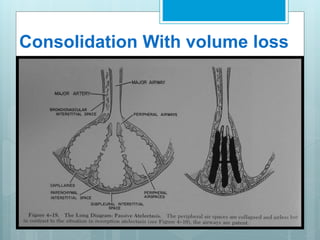
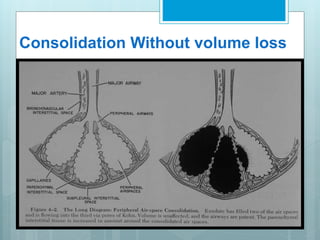
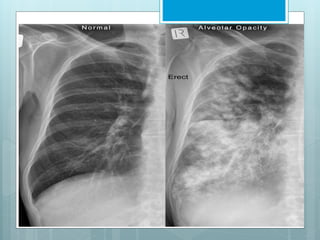
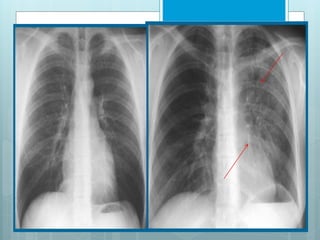
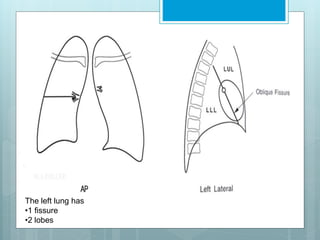
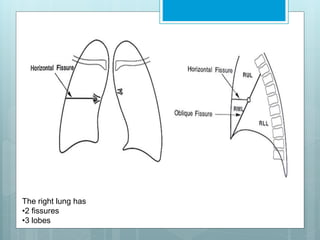
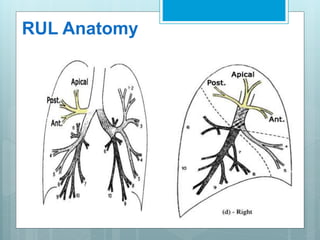
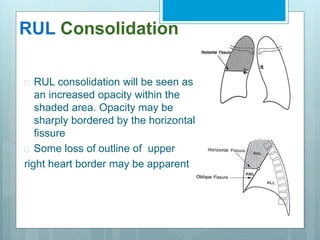
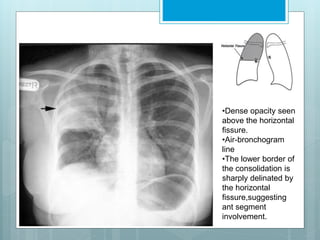
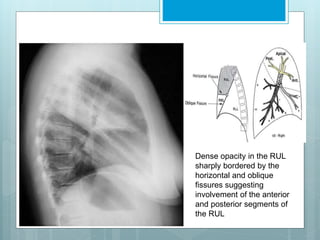
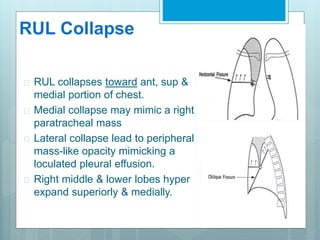
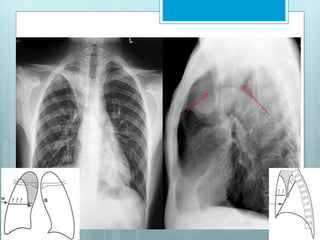
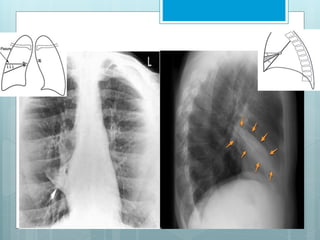
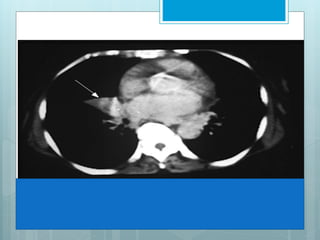
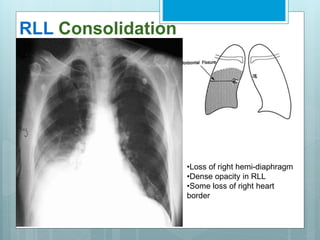
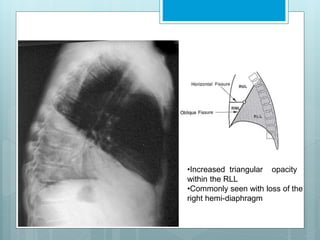
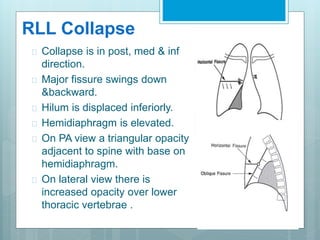
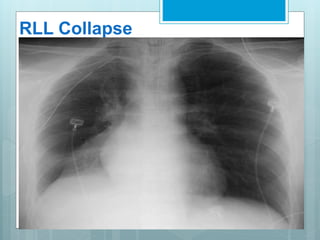
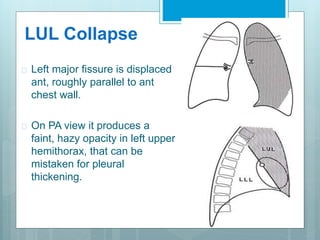
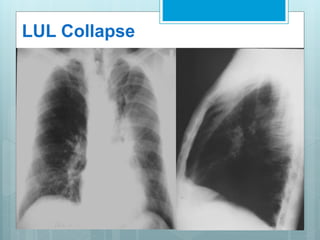
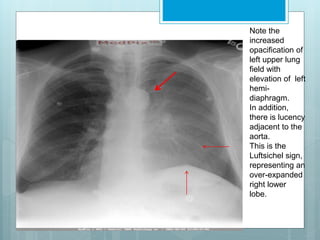
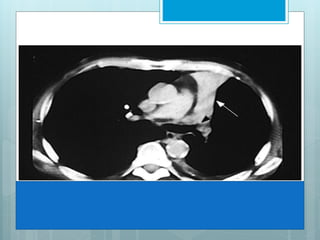
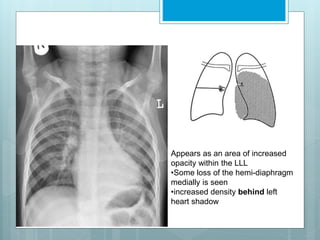
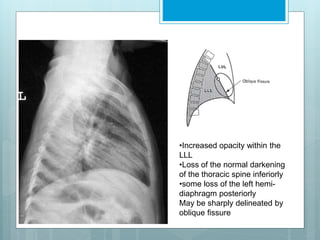
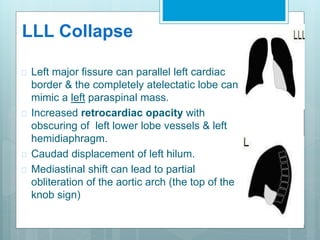
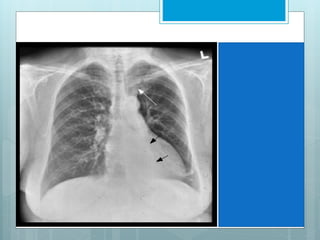
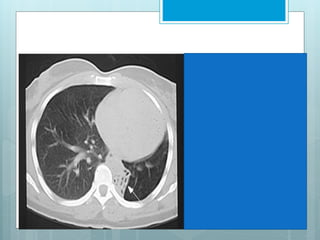
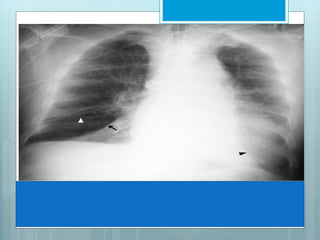
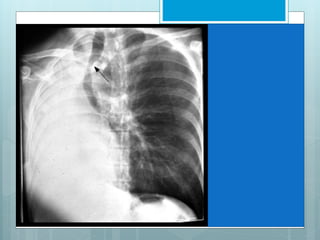
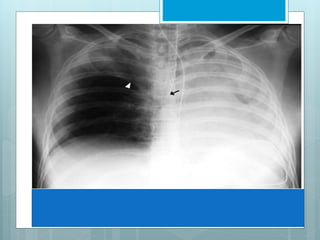
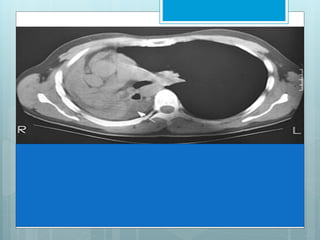
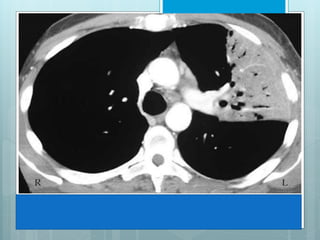
The document discusses lung collapse (atelectasis) and consolidation. Collapse is a loss of lung volume while consolidation involves fluid filling the alveoli. Collapse can be caused by obstruction of airways or loss of contact between the lungs and chest wall. Consolidation is seen in conditions like pneumonia. Specific patterns of collapse and consolidation are seen on chest x-rays depending on the affected lung lobe. Signs like fissure shifts and volume changes in the unaffected lobes help identify the collapsed lobe.