Downloaded 682 times




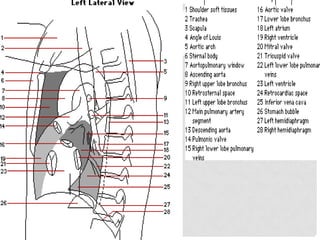














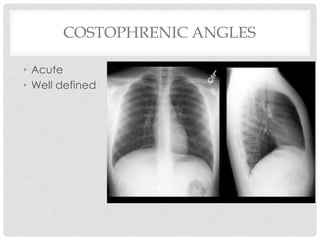
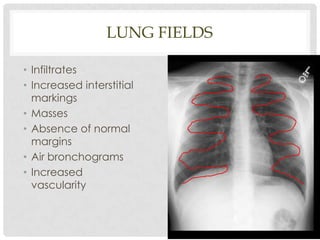











This document provides guidelines for interpreting a chest x-ray, including structures to identify, technical aspects to evaluate, and what to examine in different areas of the image. It describes how to analyze the trachea, heart, diaphragms, lungs, hilum, and other areas. Key points covered are proper centering, penetration, inspiration, and angulation of the x-ray. Anatomical landmarks are identified for assessing abnormalities in each lung field.

















































































