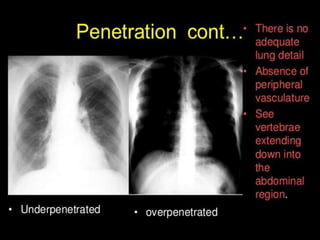
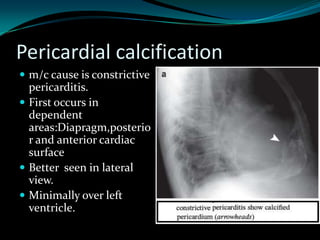
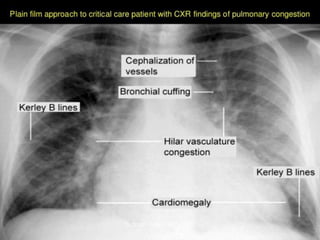
This document provides an overview of chest x-ray interpretation. It begins with a brief history of x-rays and how they are produced. It then describes how different tissues absorb x-rays differently, appearing as varying shades of gray on the image. The rest of the document details normal anatomy seen on a CXR like the lungs, heart, vessels, bones and soft tissues. It provides guidance on positioning, penetration, inspiration and technical factors. Common abnormalities are also discussed like effusions, masses, fractures and cardiac issues.