Downloaded 6,581 times
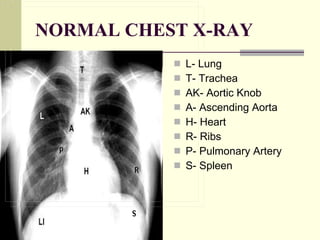
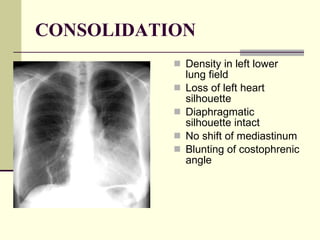
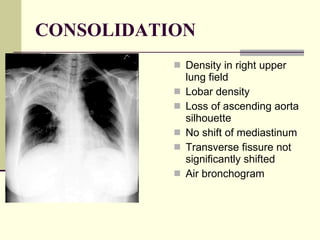
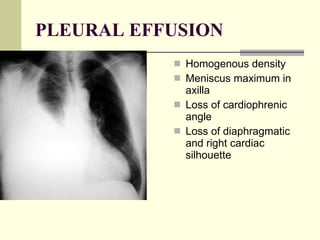
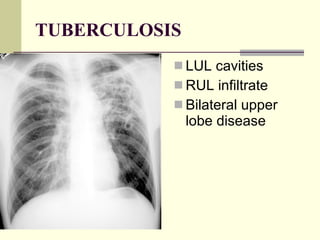
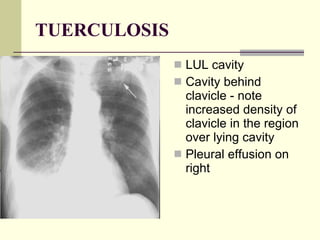
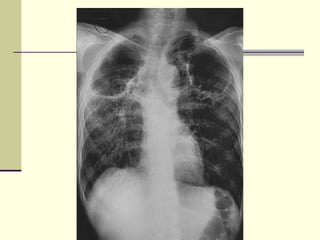
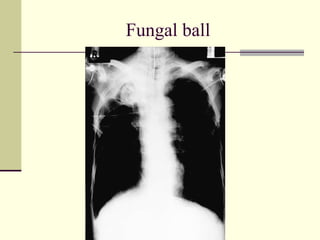
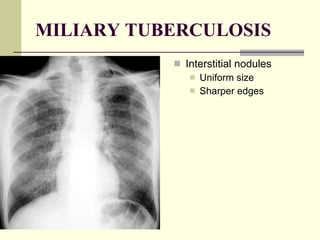
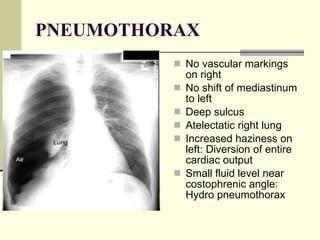
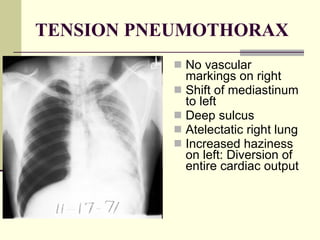
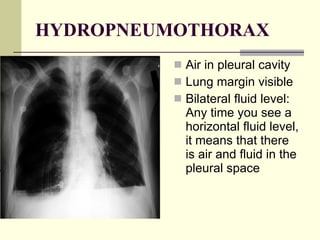
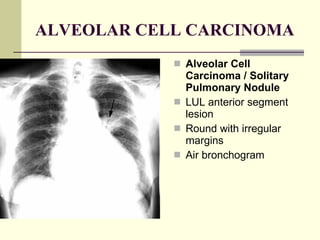
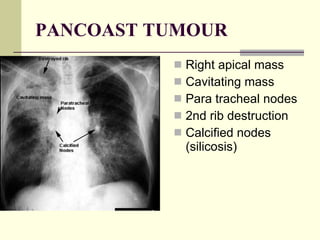

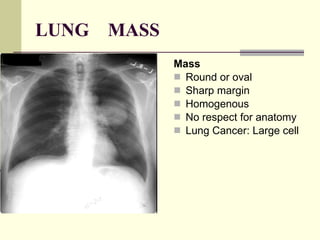
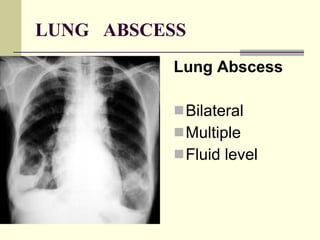
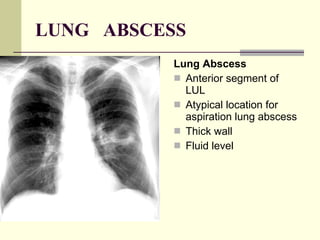
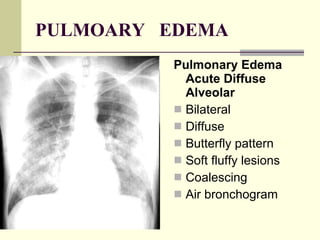


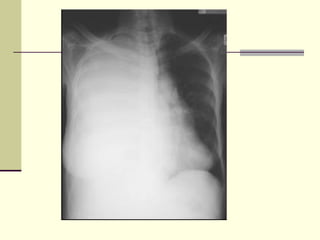

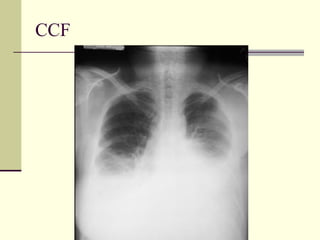
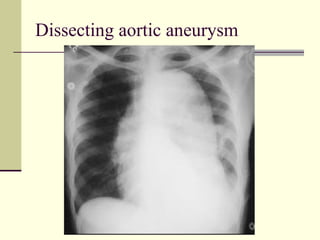



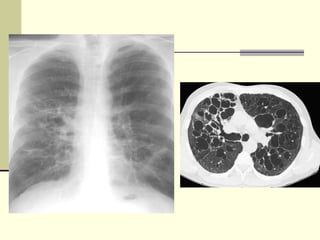
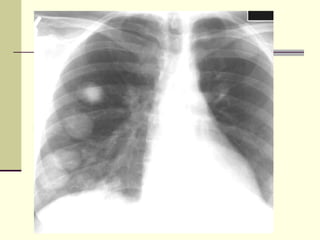

The document provides an overview of the pathology of lung diseases as seen on chest x-rays, including signs, appearances and common causes of conditions such as consolidation, pleural effusion, atelectasis, pneumothorax, lung masses, fibrosis and infections like tuberculosis. Differential diagnoses are also provided for various lung abnormalities seen on x-rays.


















































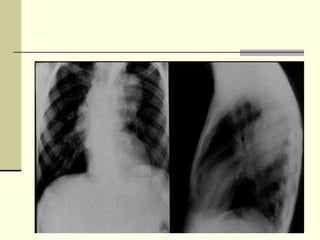
![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















