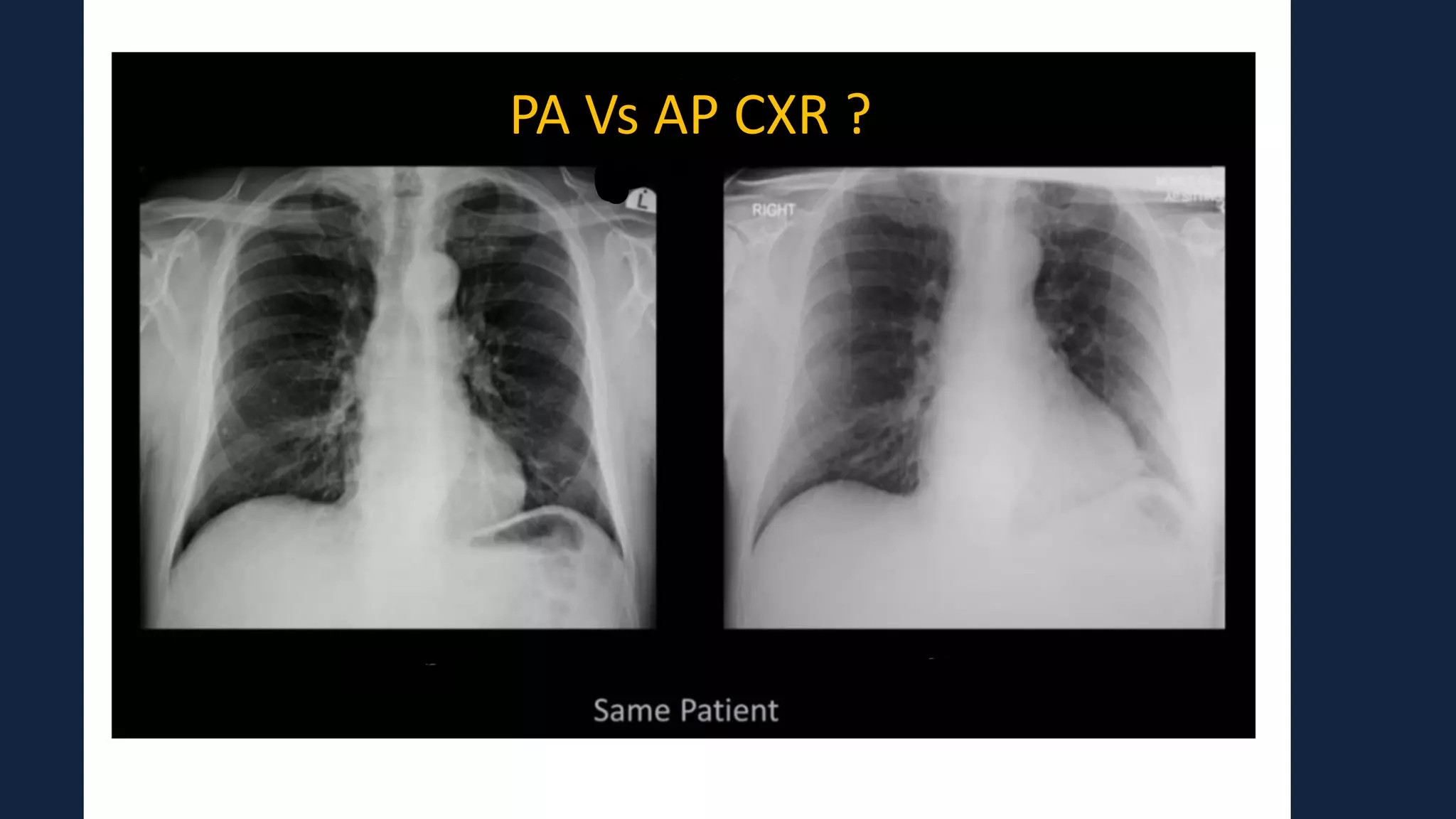
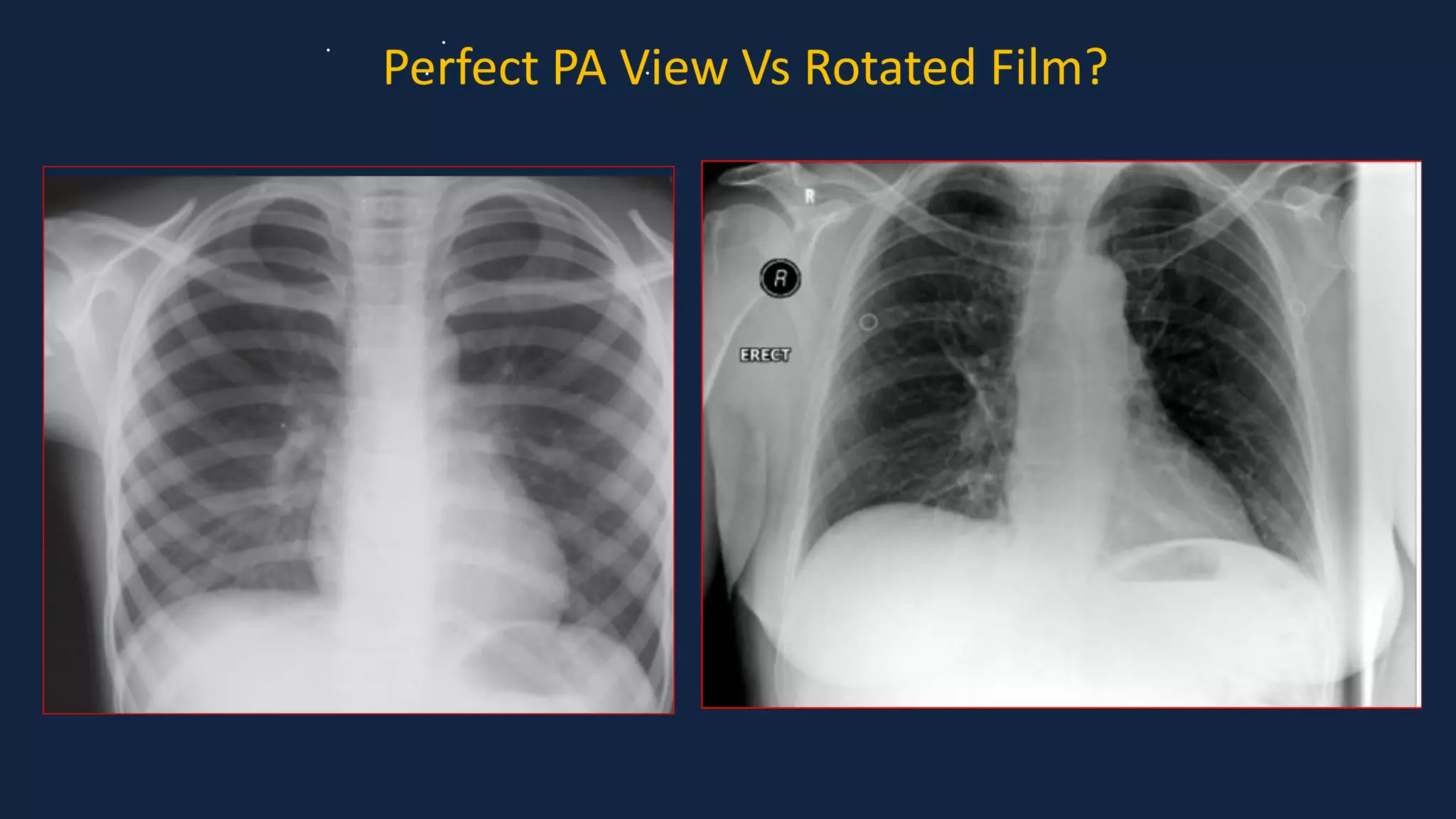
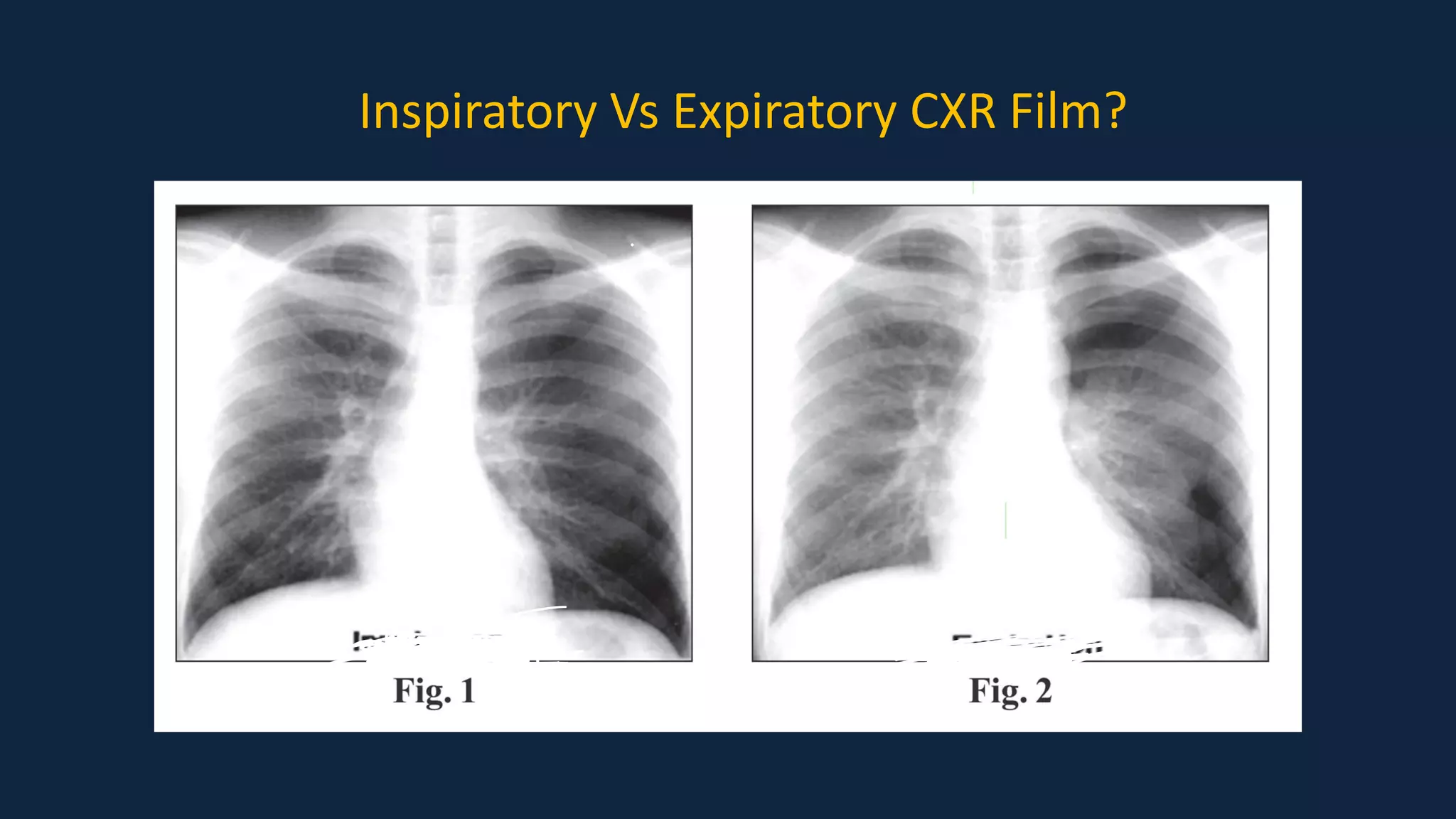
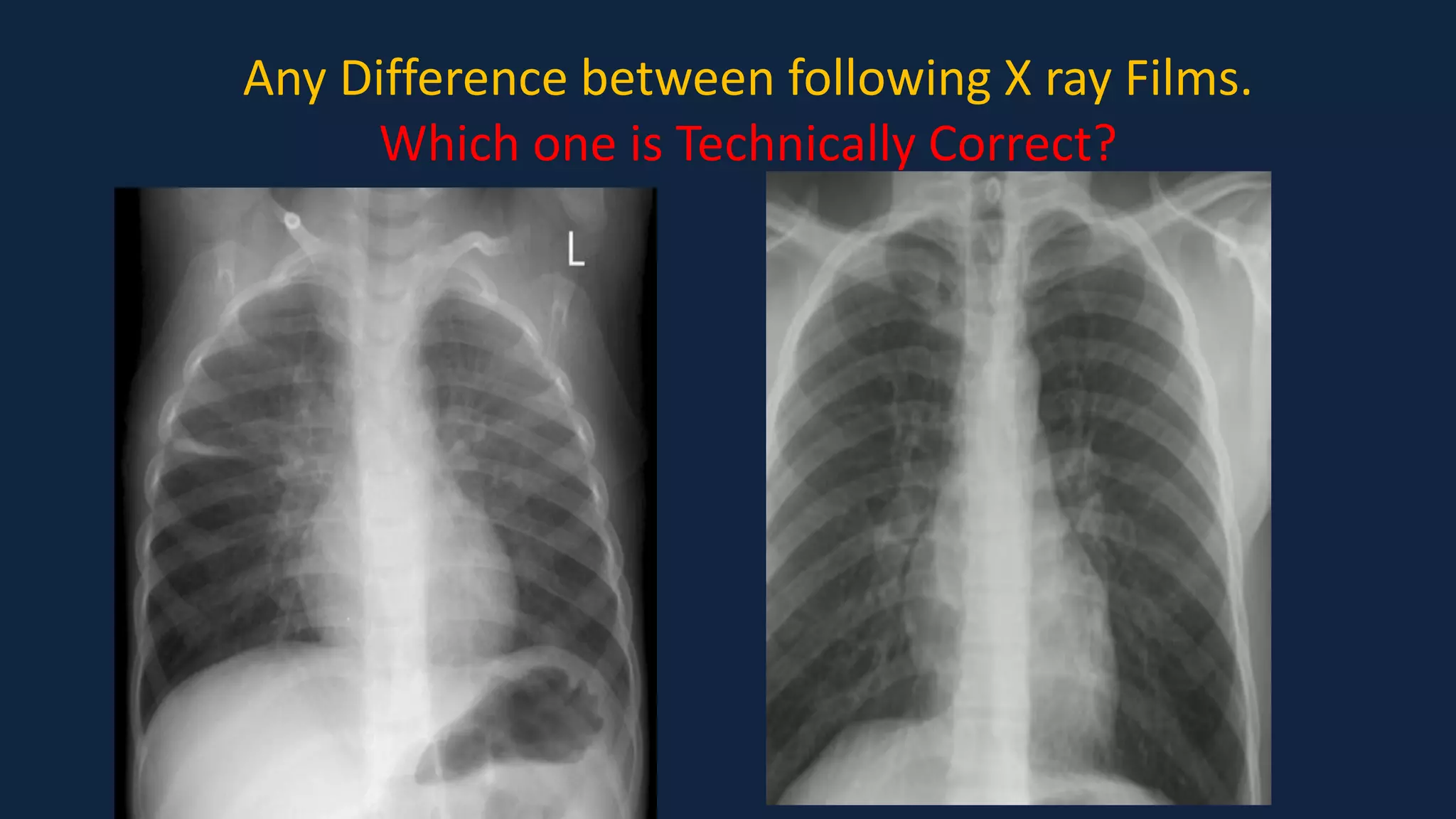
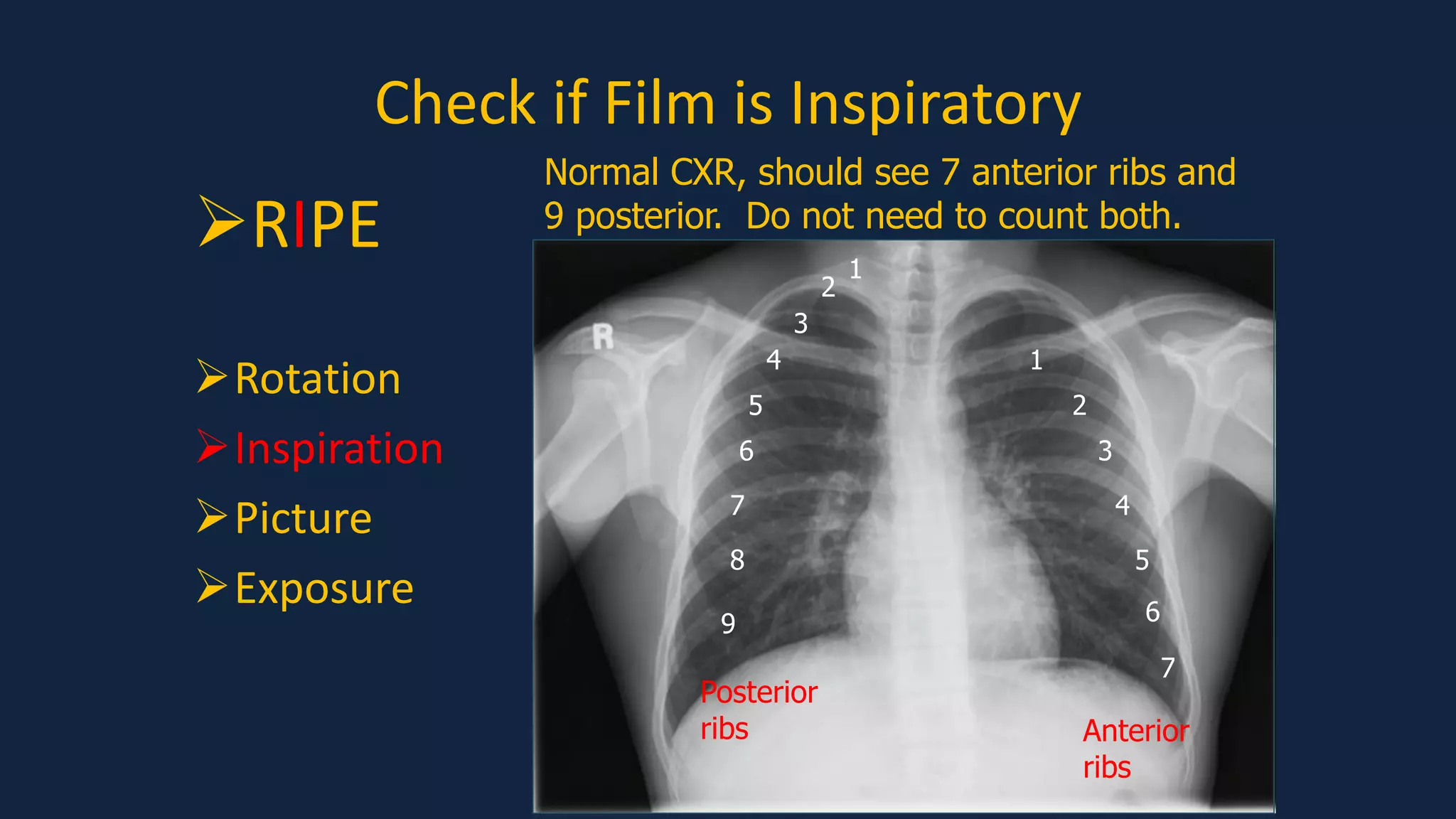
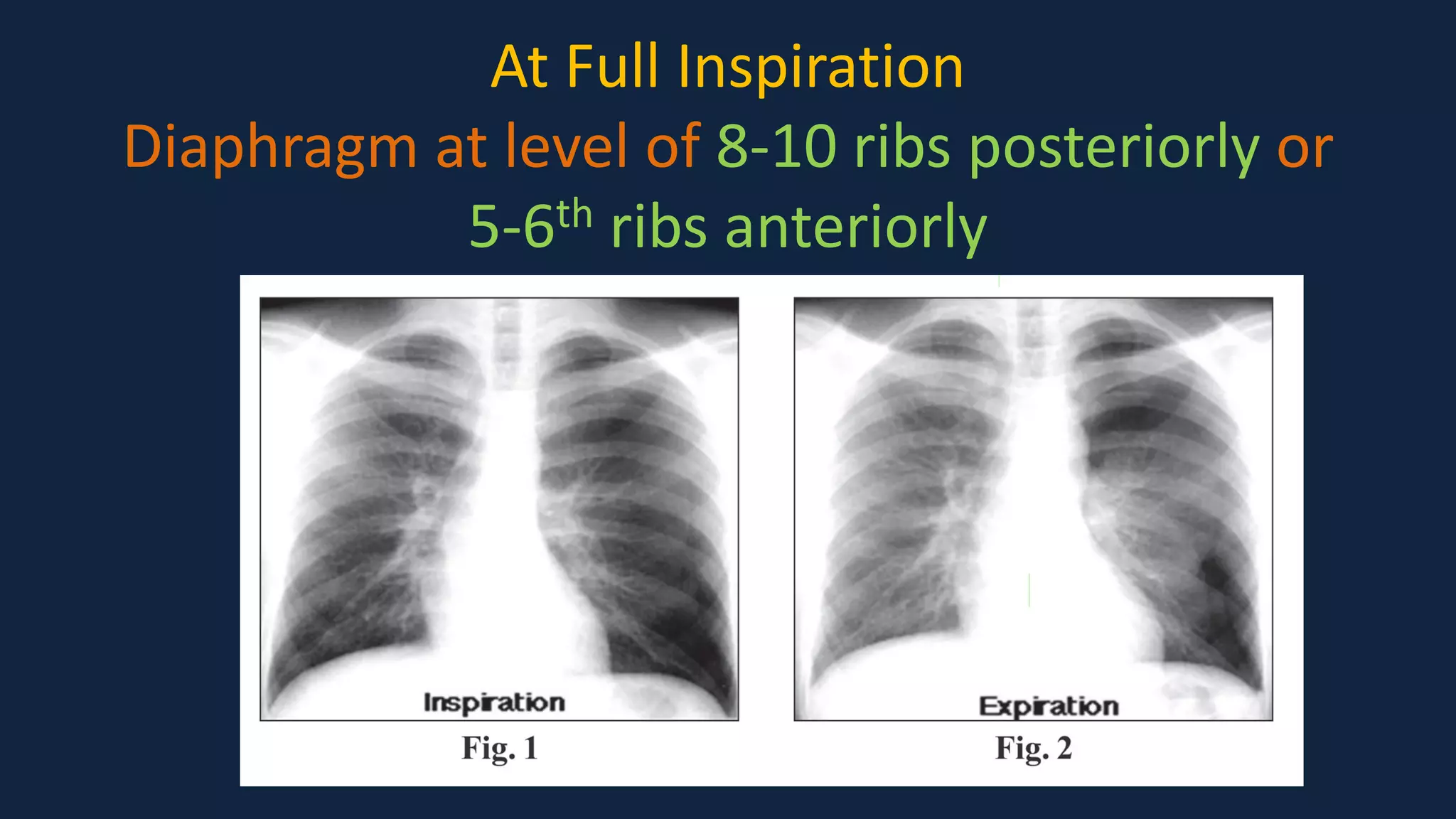
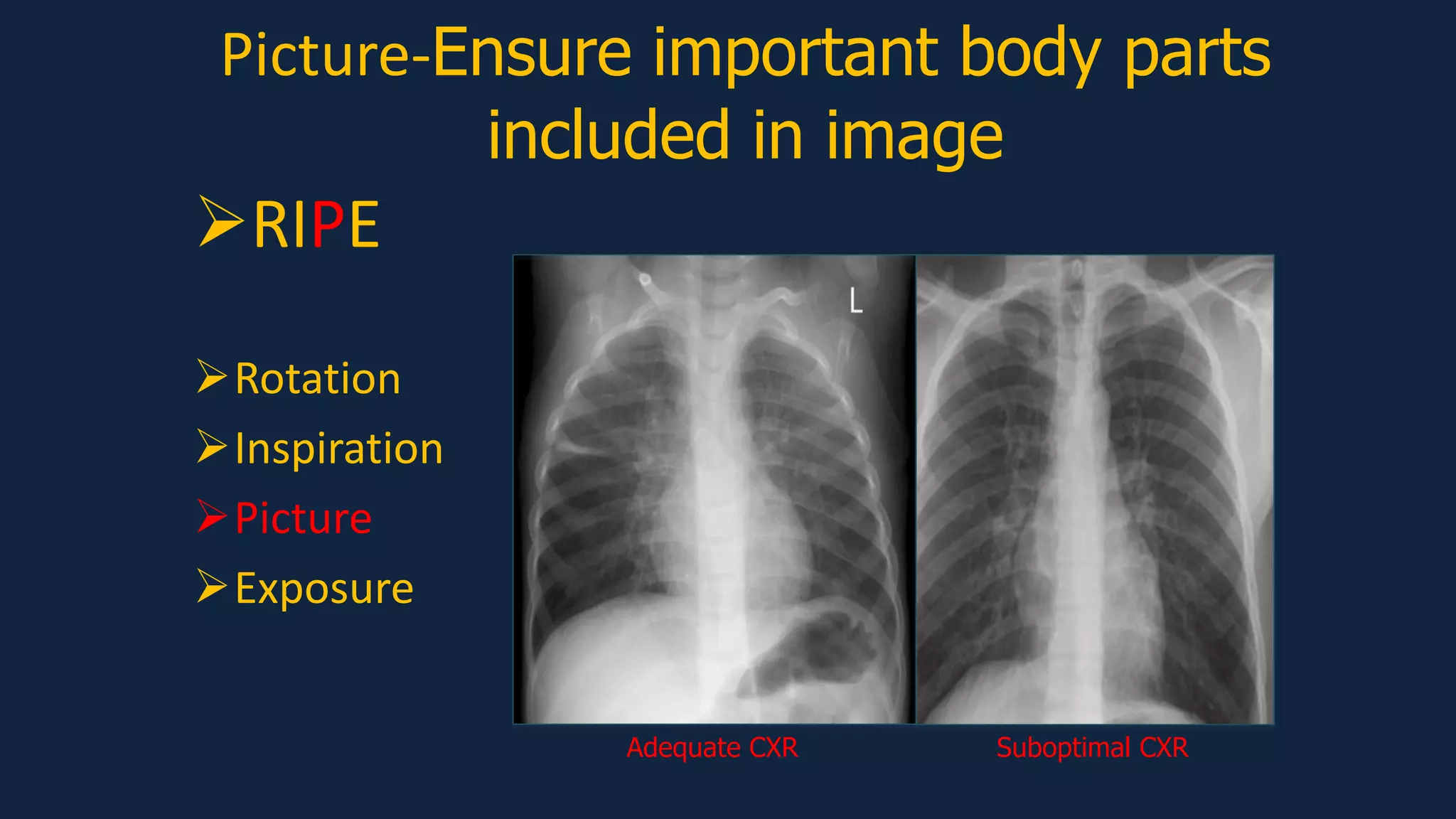
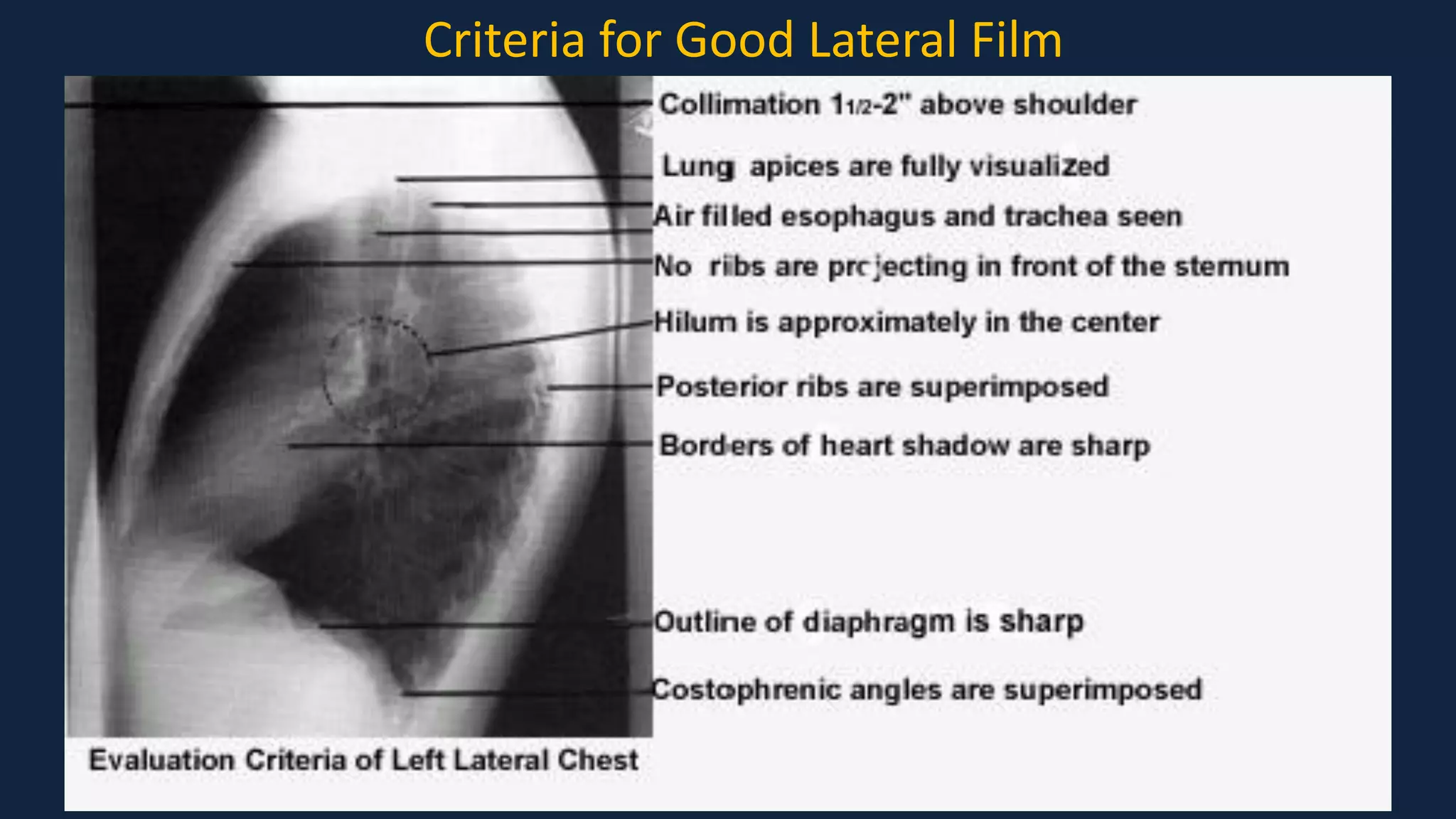
This document provides guidance on systematically interpreting pediatric chest x-rays. It discusses evaluating rotation, inspiration, image quality and exposure. It describes analyzing the cardiac silhouette, lungs, diaphragm and hidden areas. Common abnormalities like consolidation, atelectasis, effusion and pneumothorax are presented. Interpreting neonatal chest x-rays involves assessing lung volumes, air bronchograms and complications of prematurity. The document emphasizes using anatomical landmarks and silhouette signs to detect subtle findings and avoid overlooking areas. It aims to equip readers with a standardized approach for accurate chest x-ray interpretation in pediatrics.