Downloaded 3,980 times



![• Juxtaphrenic peak sign
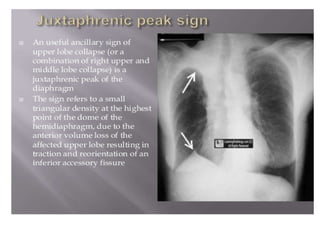
• The juxtaphrenic peak sign, which occurs in upper lobe
atelectasis, describes the triangular opacity projecting
superiorly at the medial half of the diaphragm (Fig. 13). It
is most commonly related to the presence of an inferior
accessory fissure[7]. The mechanism is not known with
certainty; according to one theory, the negative pressure
of upper lobe atelectasis causes upward retraction of the
visceral pleura, and protrusion of extrapleural fat into the
recess of the fissure is responsible[15]. The juxtaphrenic
sign can also be seen in combined right upper and
middle lobe volume loss or even with middle lobe
collapse only.](https://image.slidesharecdn.com/collapseandconsolidation1-131030064603-phpapp01/85/Collapse-and-consolidation-Lung-Radiology-24-320.jpg)
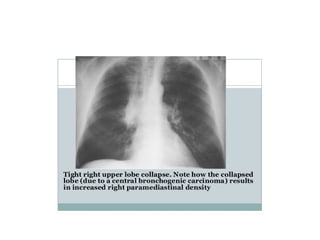
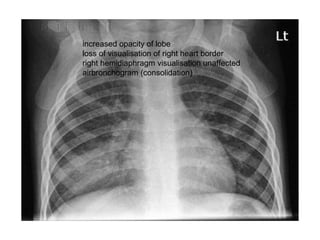

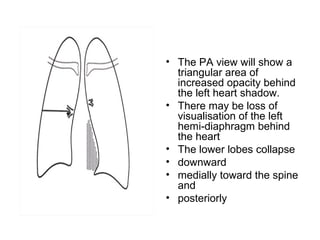

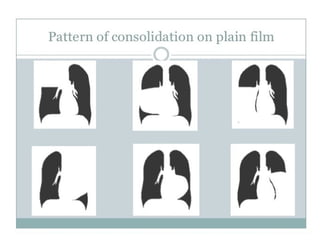
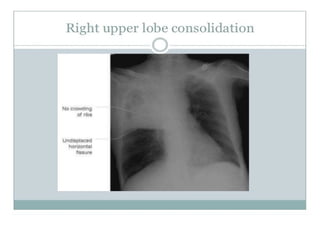
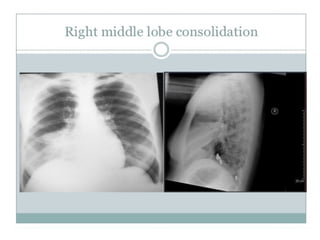
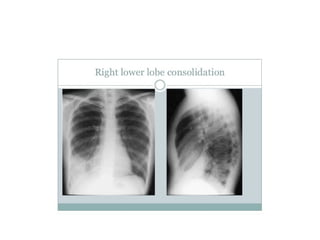
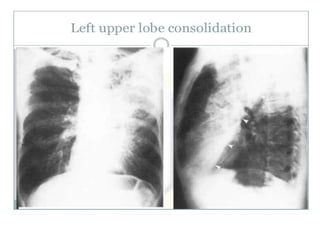
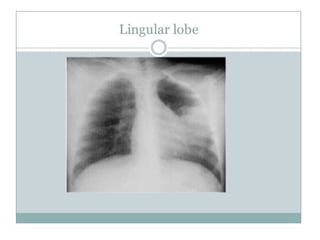
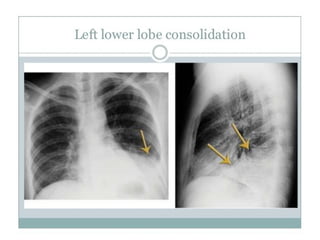
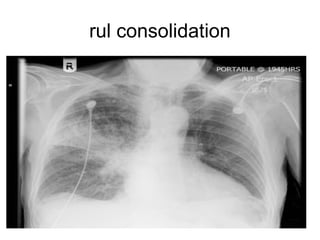


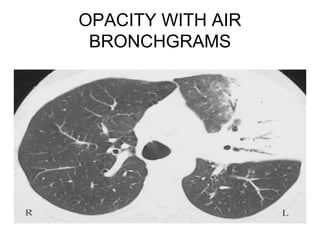


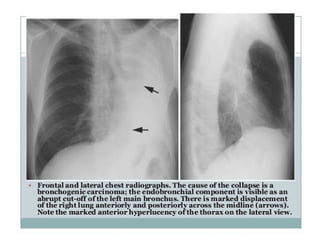
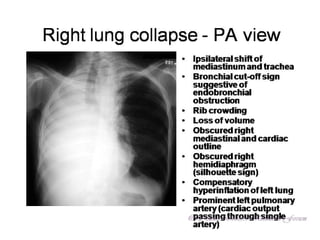
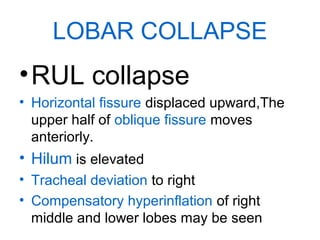
1) The document discusses mechanisms, patterns, and radiological signs of lung collapse and consolidation. It describes how collapse is diminished lung volume with reduced volume, while consolidation has normal lung volume with replacement of air. 2) Common patterns of lung collapse discussed include complete, lobar (right upper, middle, lower, left upper, lingula), and signs include fissure displacement, vascular changes. Consolidation causes opaque lung tissue and may show air bronchograms if airways are patent. 3) CT and ultrasound are also useful, with ultrasound showing echogenic consolidated lung tissue without normal air shadows. Key signs of specific lobar collapses and consolidations are described.























































































