Downloaded 203 times






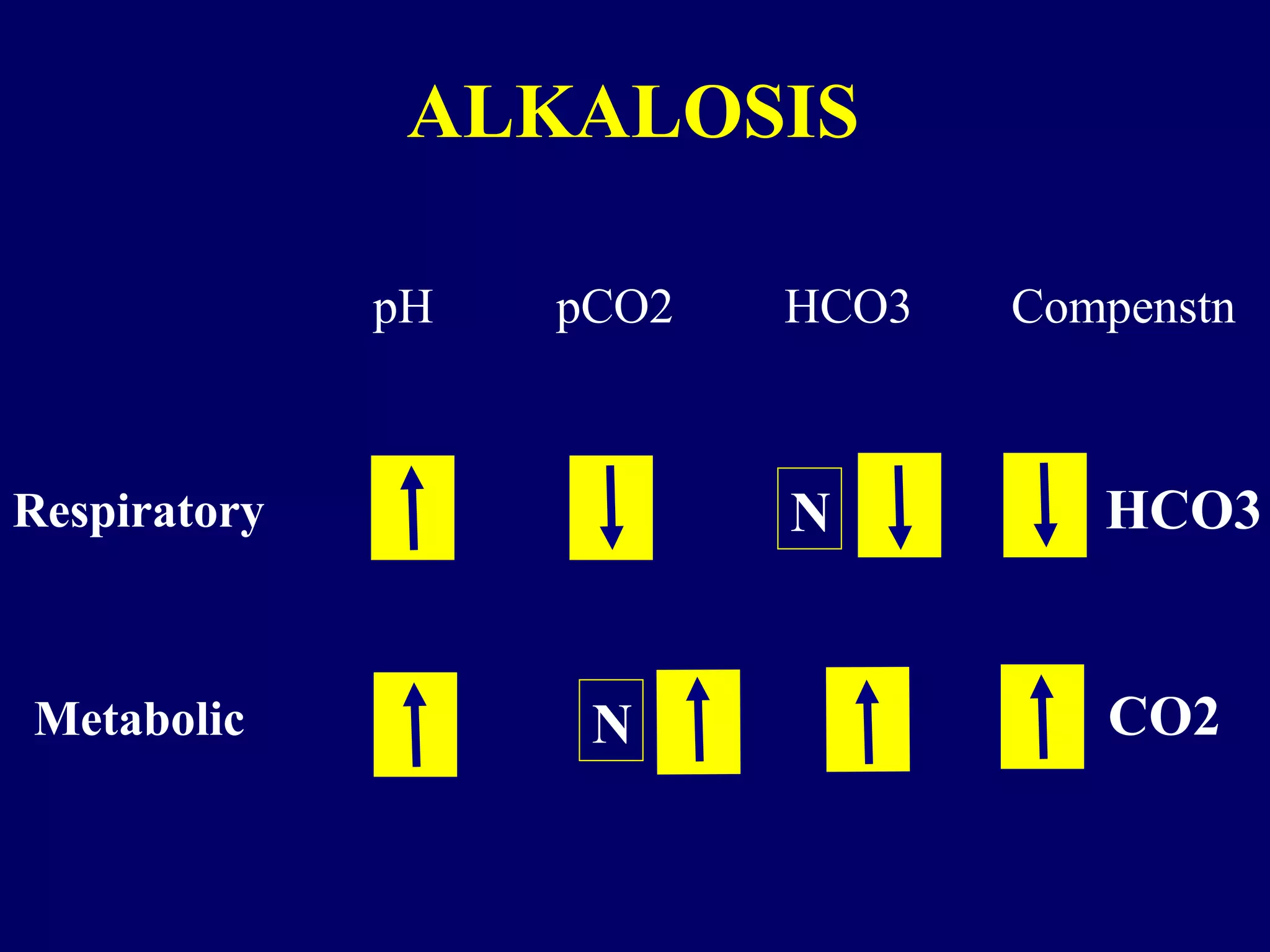






























This document discusses arterial blood gas (ABG) analysis and interpretation. It covers: - Why ABGs are important for clinical insight and picking up issues like hypercarbia that pulse oximetry cannot. - Key principles like acid-base balance, recognizing simple vs. complex disorders. - When to request ABGs, such as for serious illness, respiratory distress, or suspected metabolic issues. - Factors that can influence ABG results like medications, electrolytes, and compensation time. - Ten "commandments" for proper ABG technique, analysis, and interpretation in the clinical context. - Several case examples are presented and analyzed to demonstrate applying the commandments.





























































![ABG[1].pptx BY DR BHAWNA ESI PGIMSR, BASAIDA](https://cdn.slidesharecdn.com/ss_thumbnails/abg1-250915145144-de471f3c-thumbnail.jpg?width=640&height=640&fit=bounds)