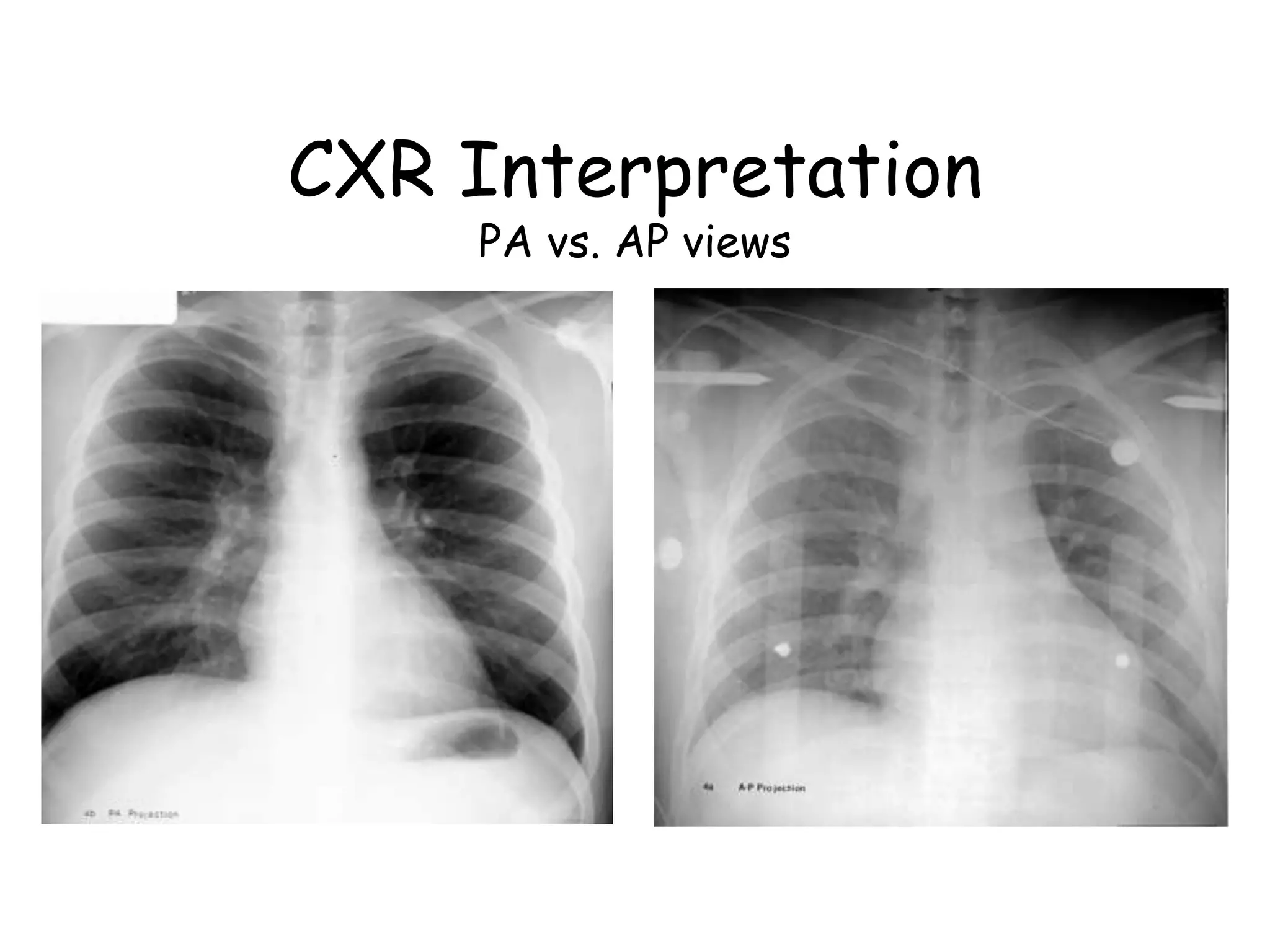
The document outlines the procedures and considerations for interpreting chest X-rays, including patient positioning, evaluation of lung fields, heart size, and diaphragm shape. It details the assessment of various conditions like pneumonia, pneumothorax, pleural effusion, and emphysema through X-ray images. Key points include recognizing normal anatomical features, identifying abnormalities, and using systematic approaches to diagnose lung and heart-related issues.