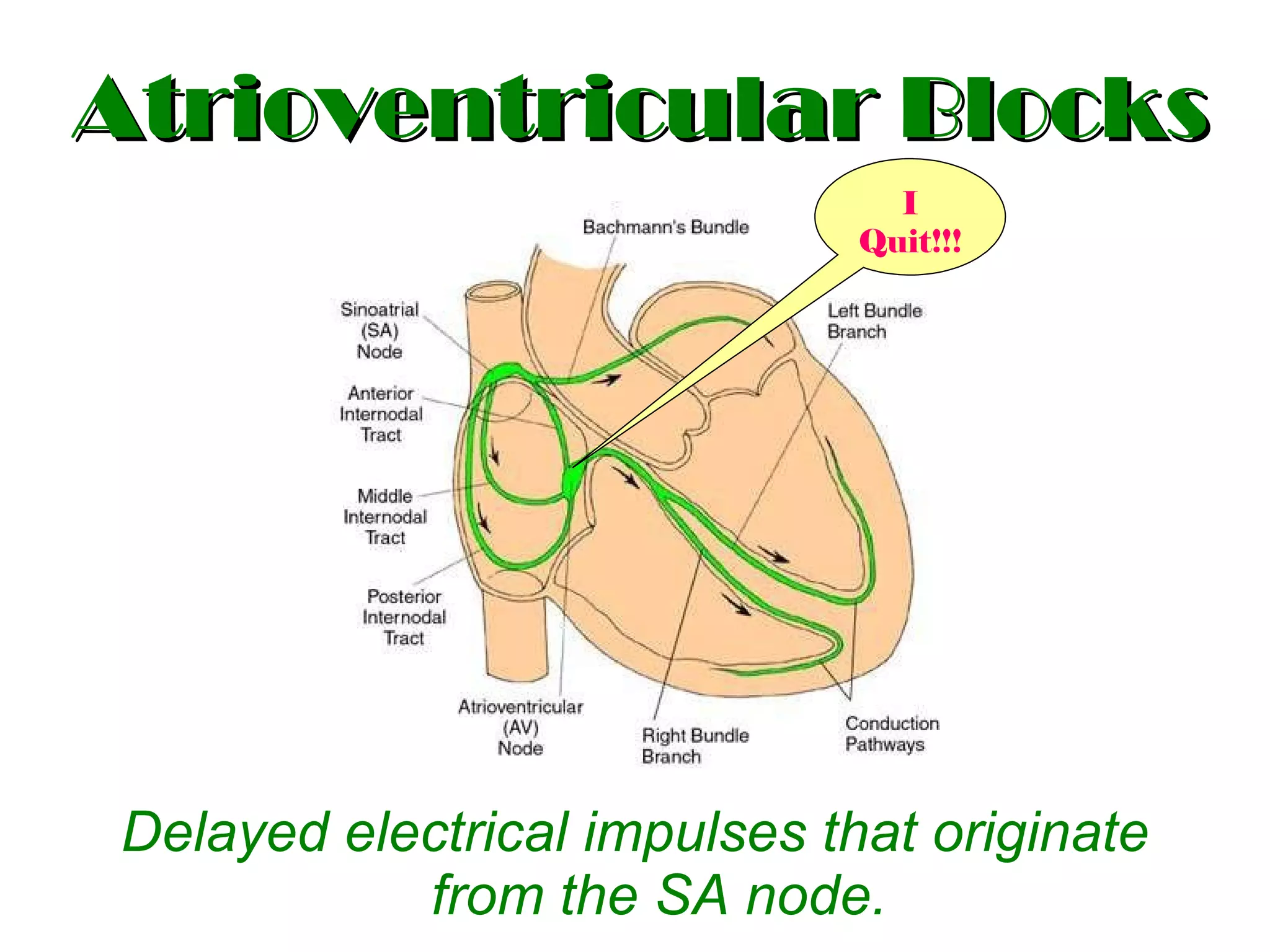
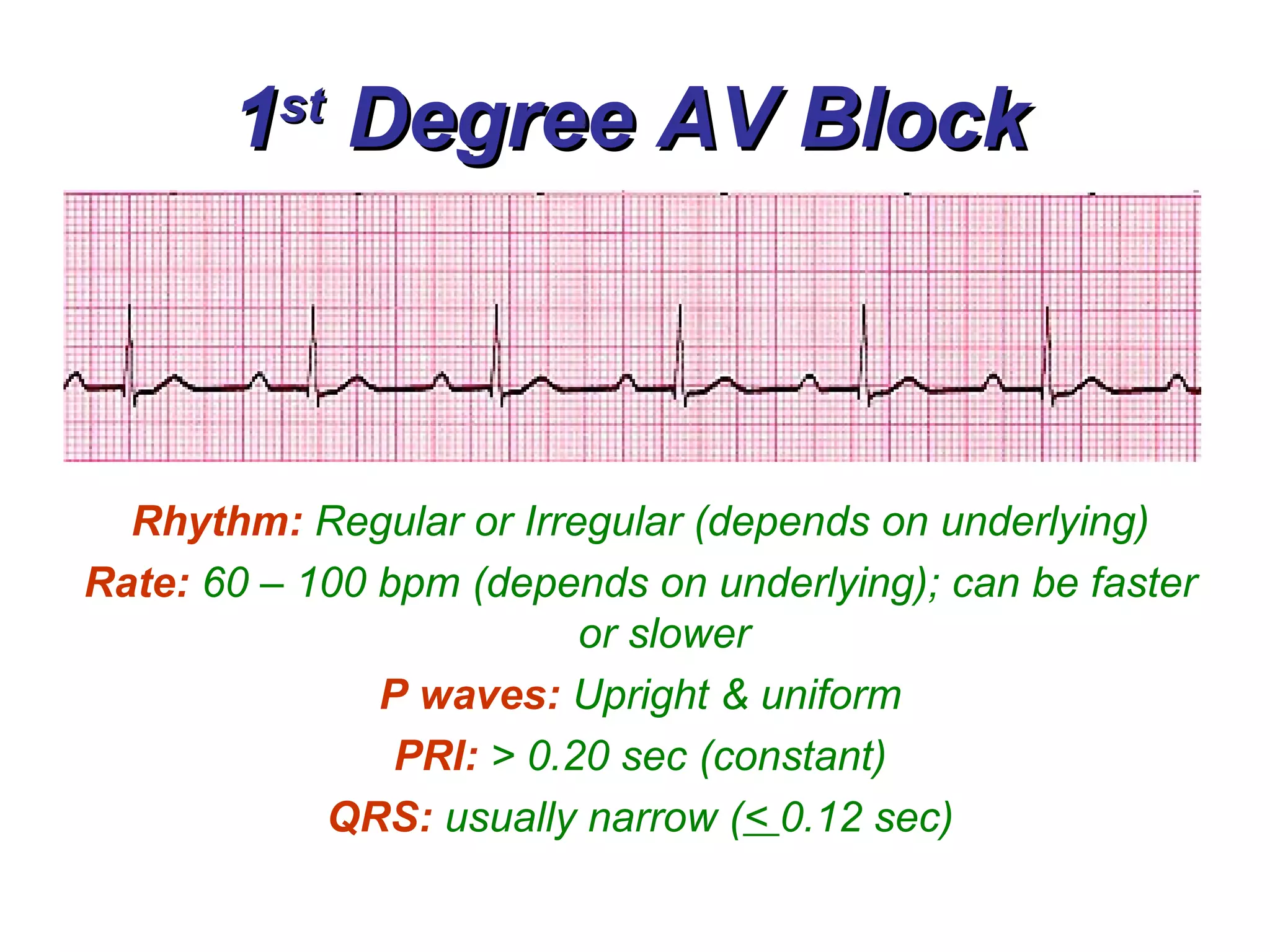
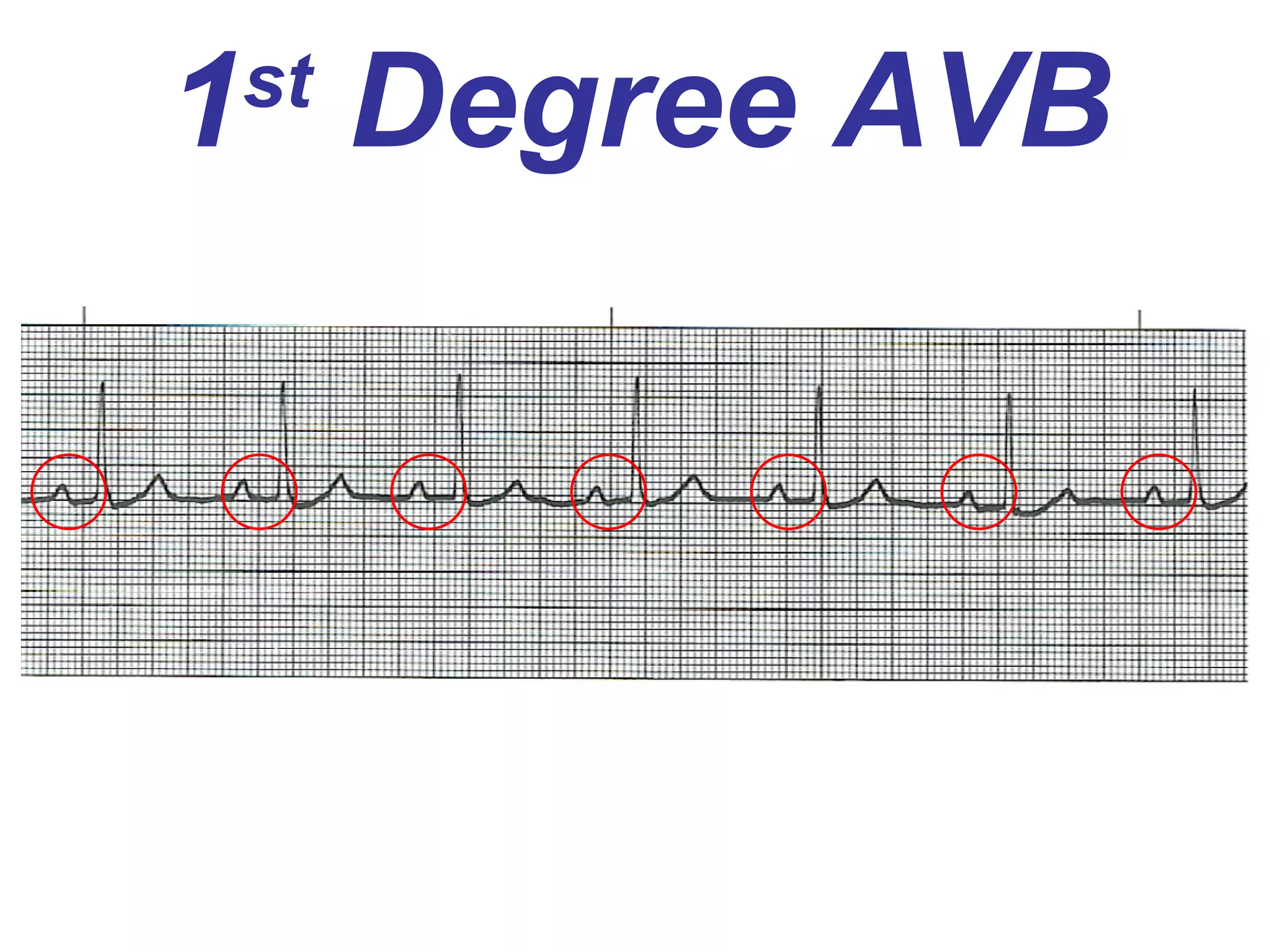
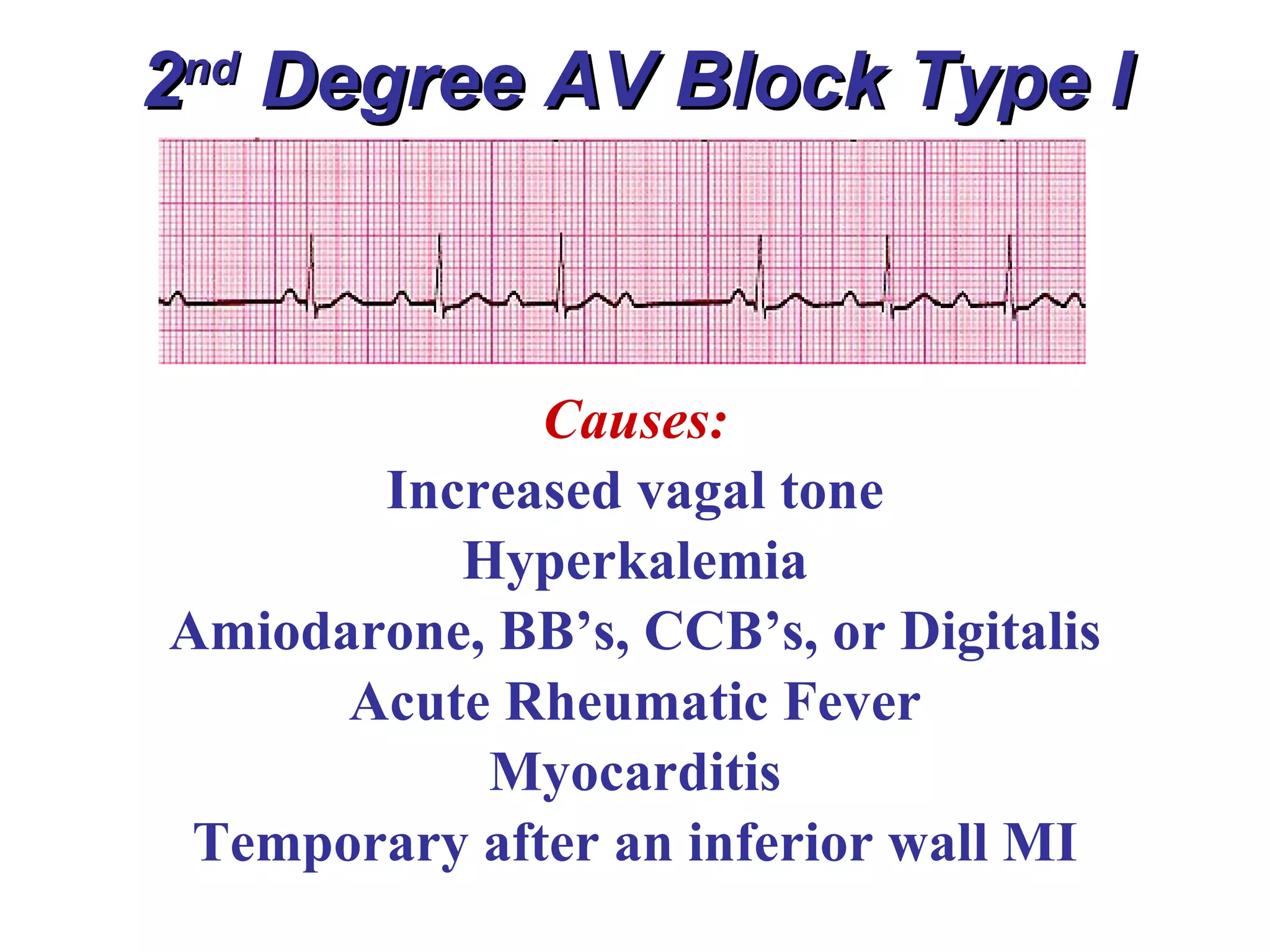
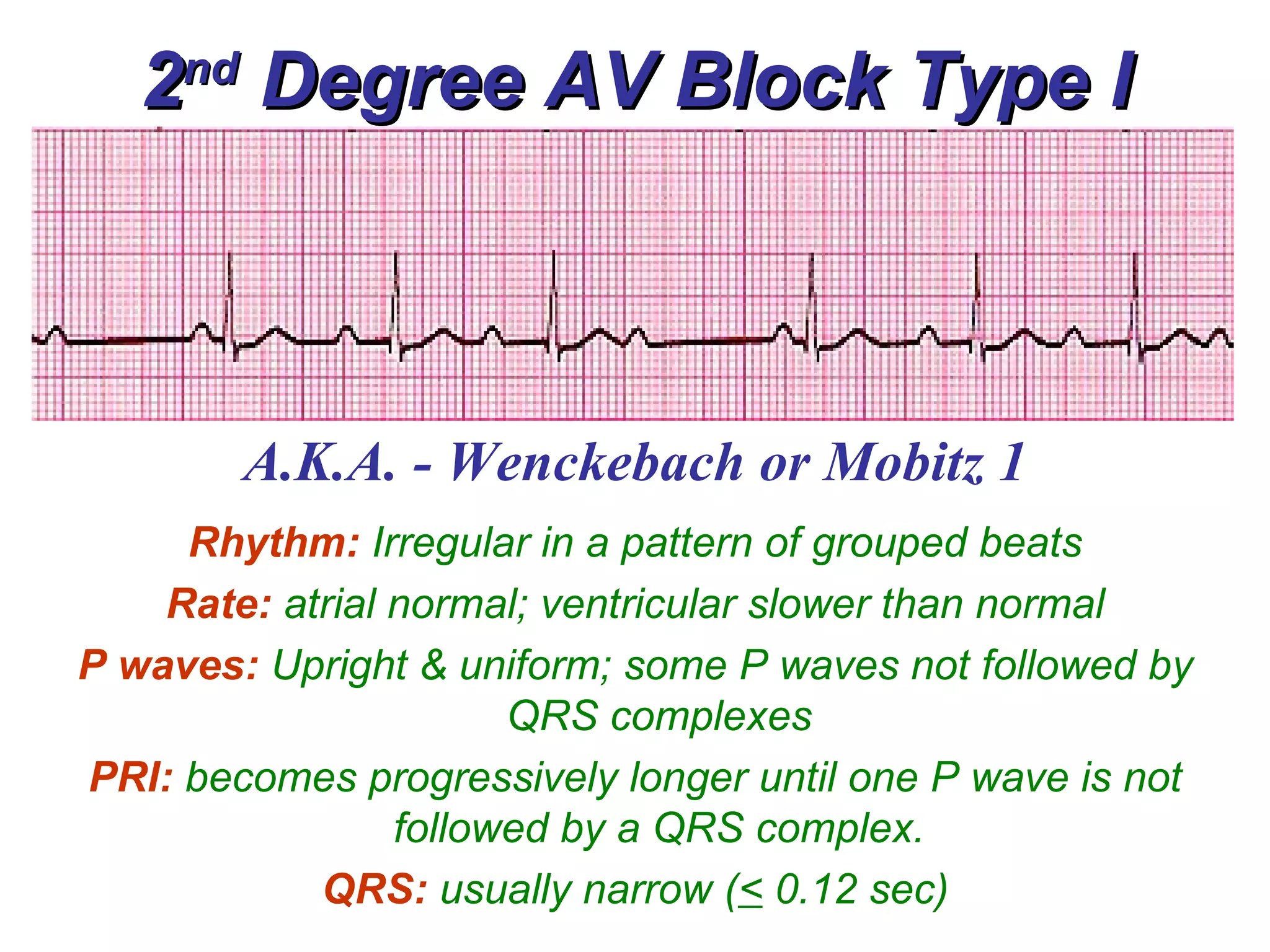
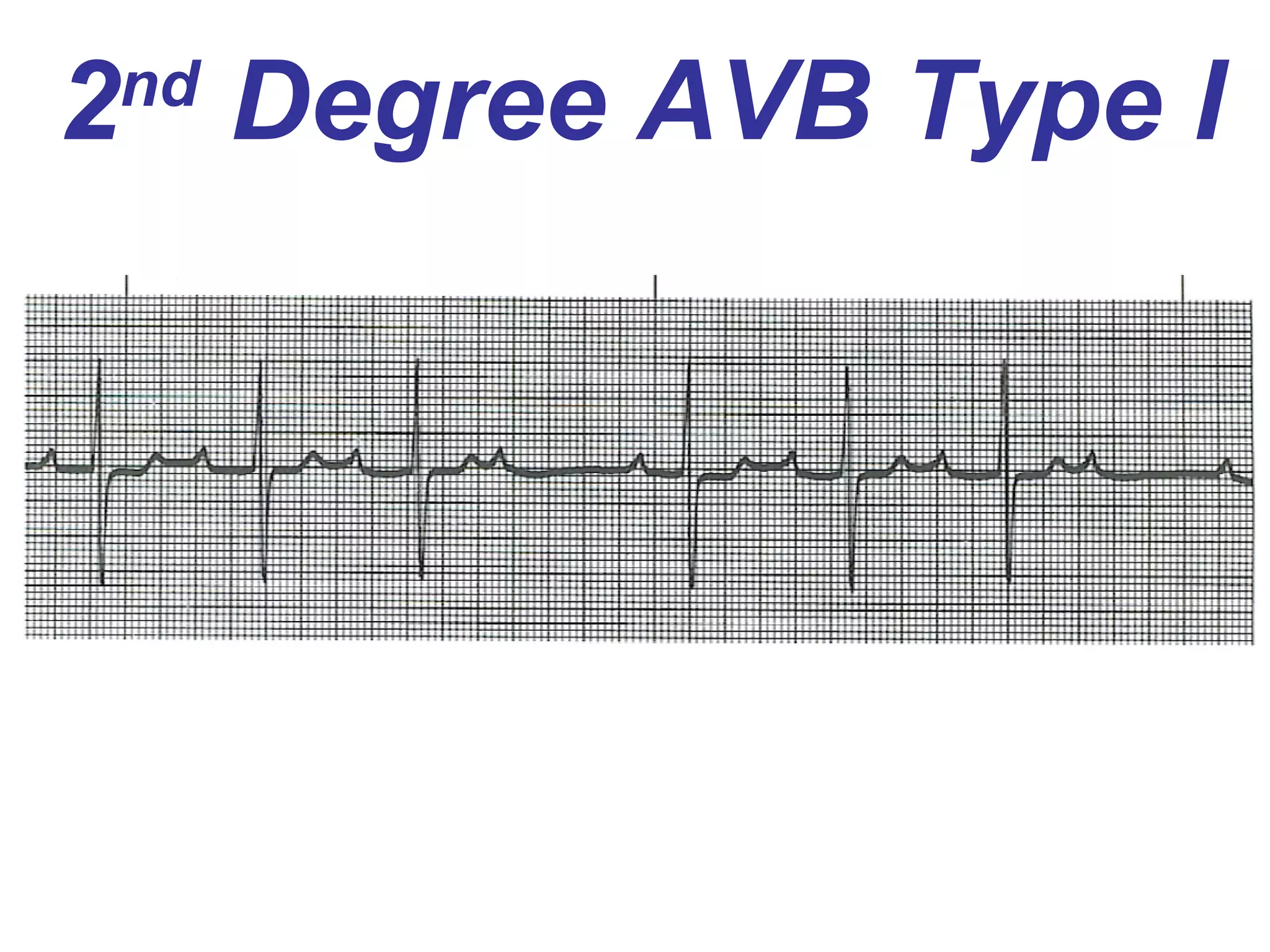
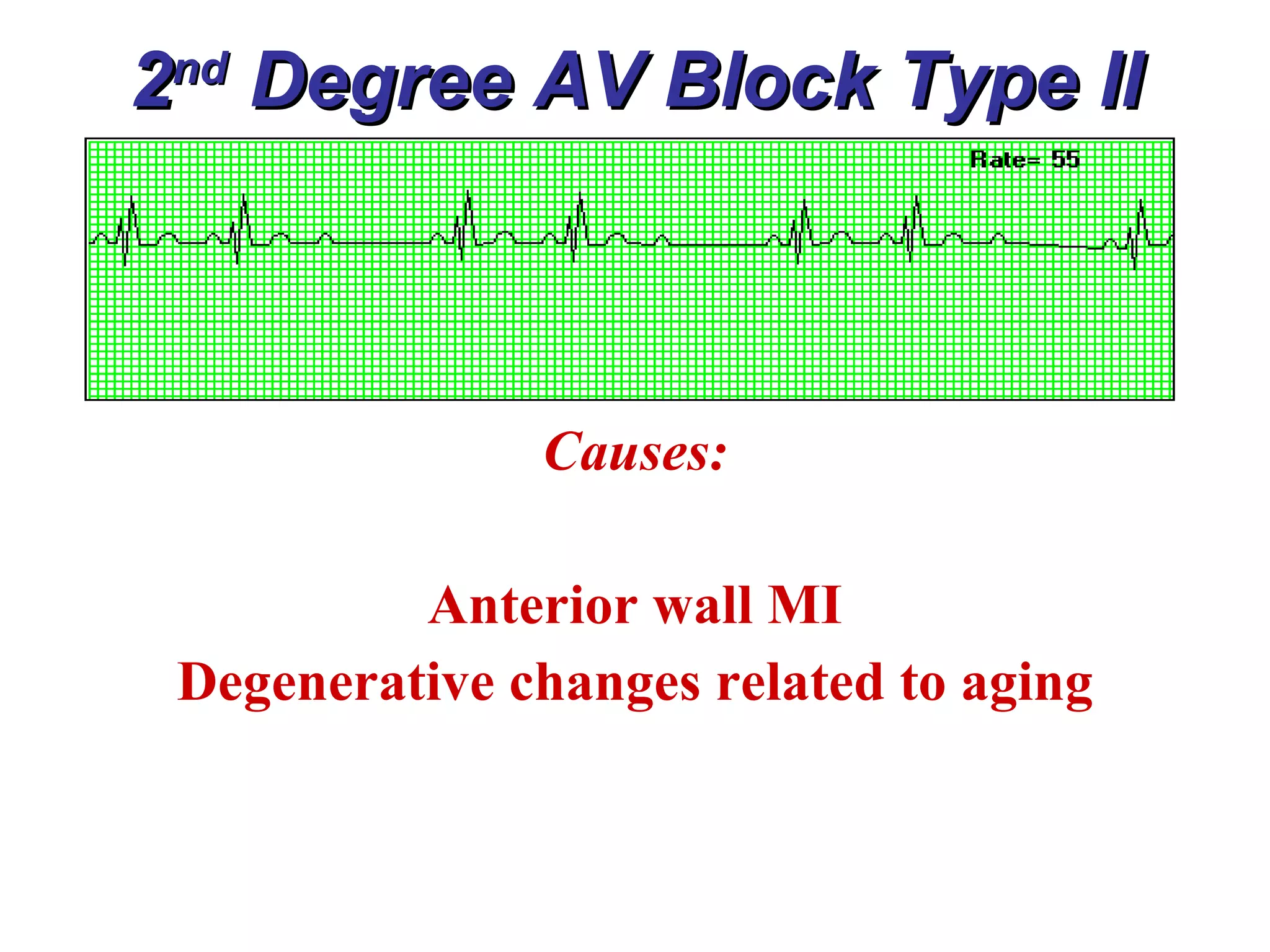
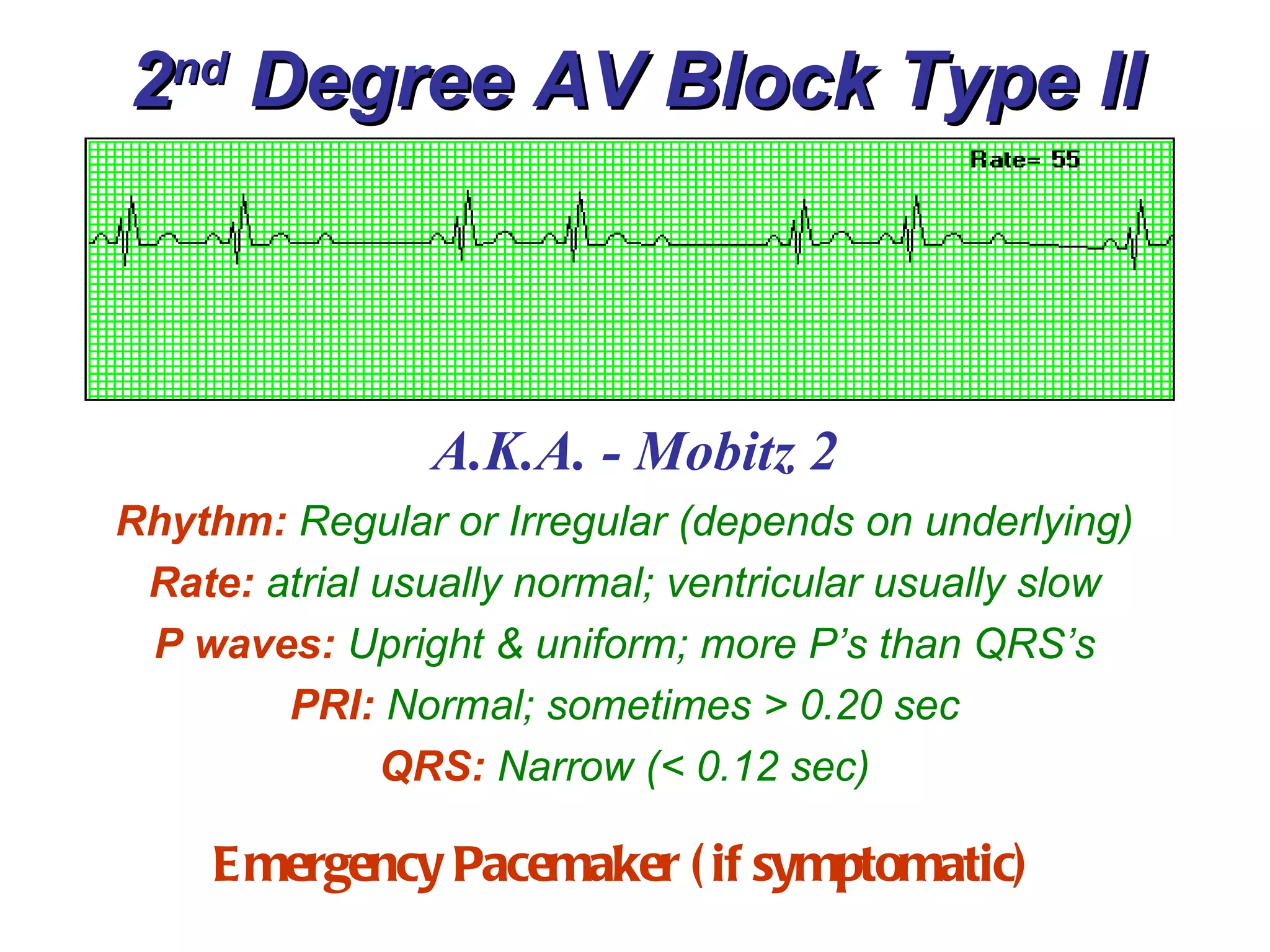
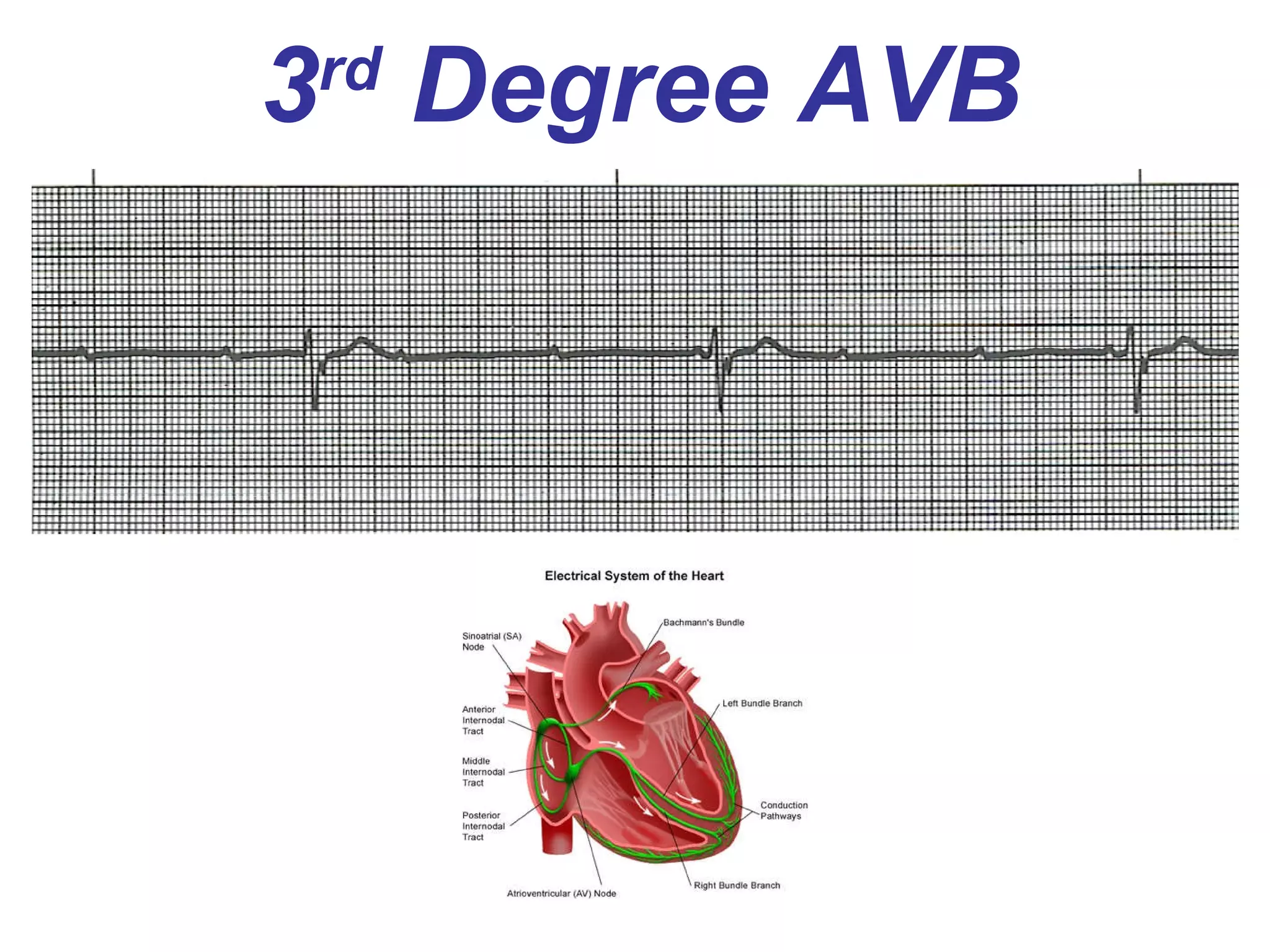
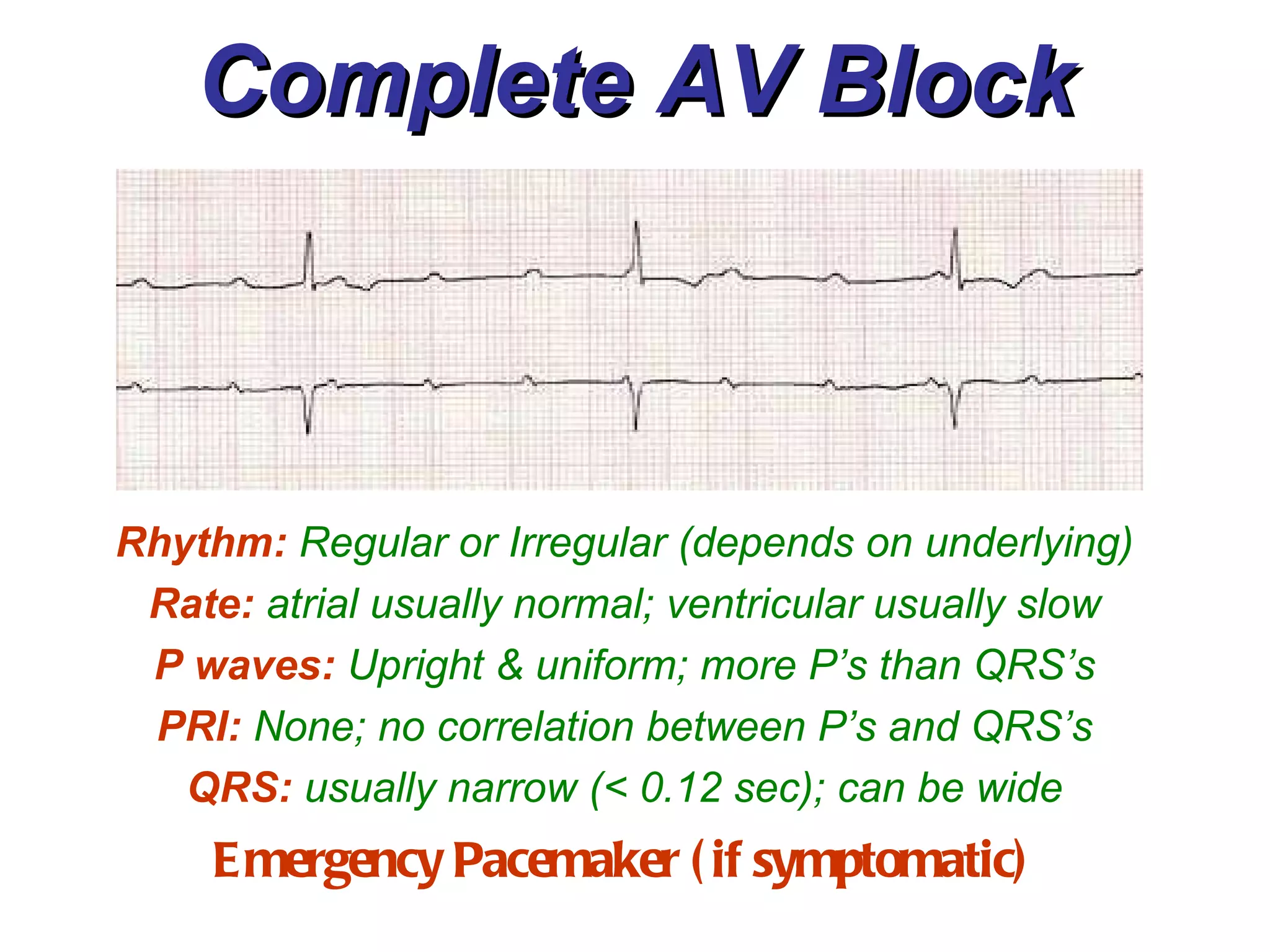
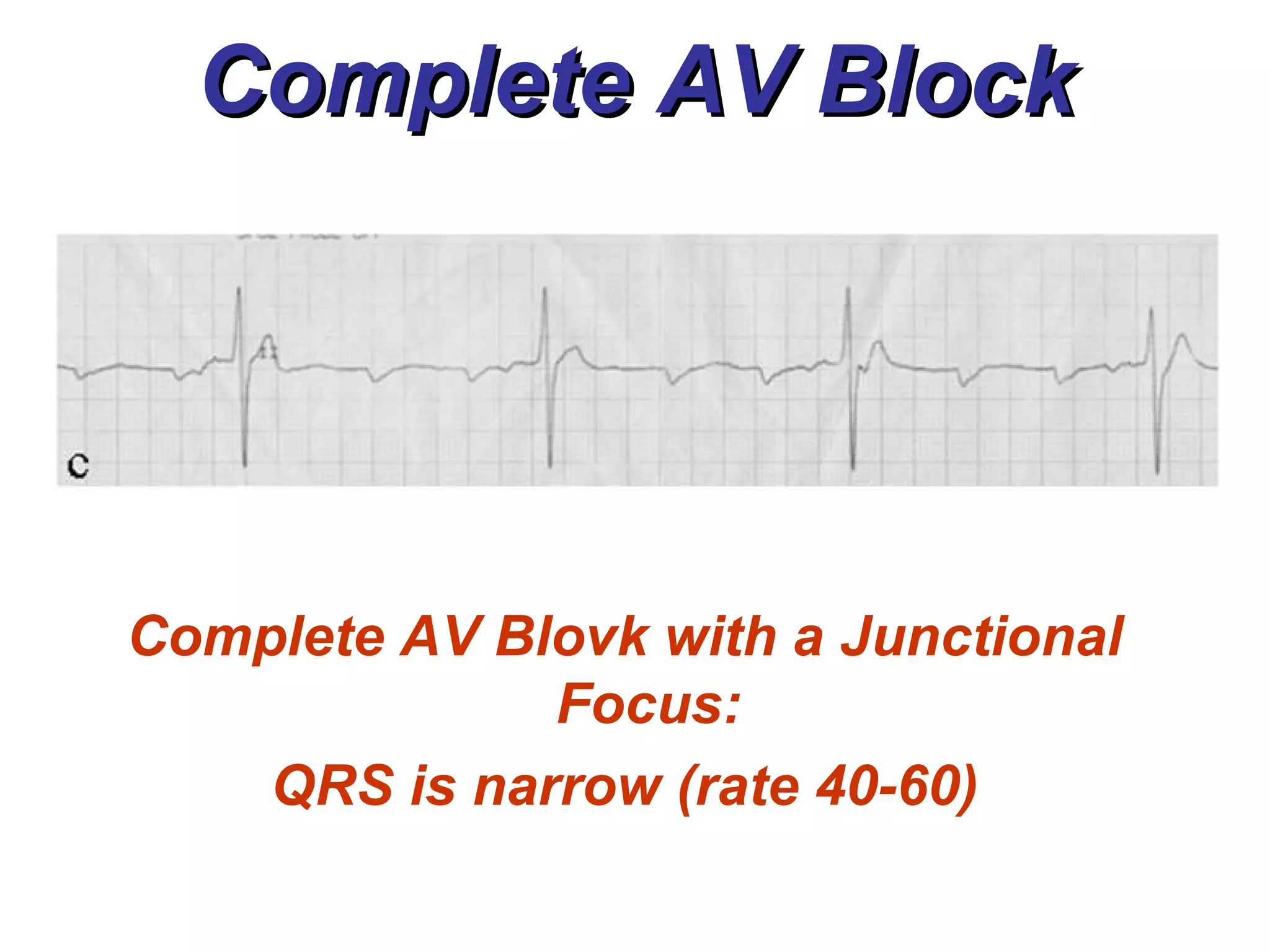
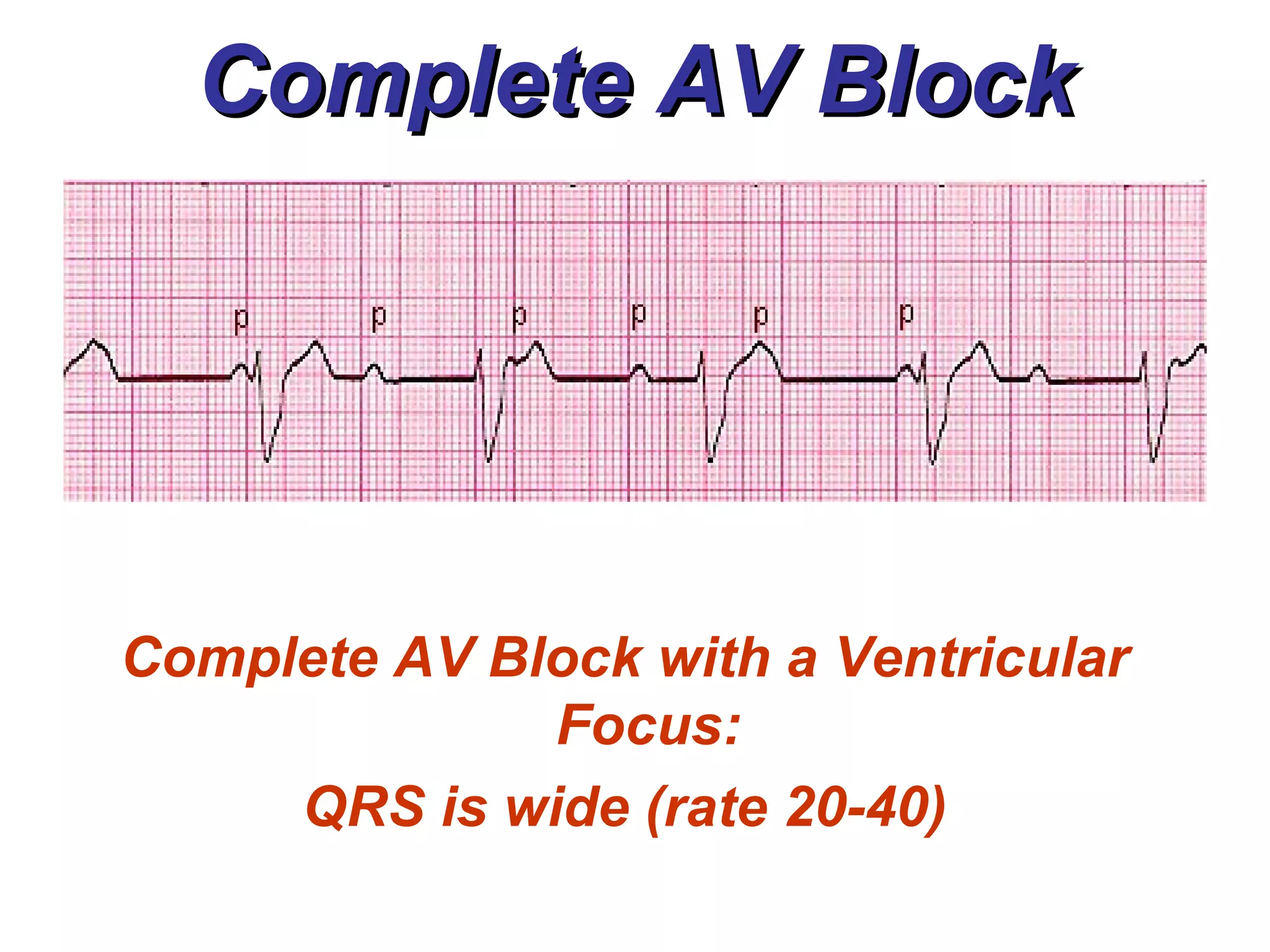
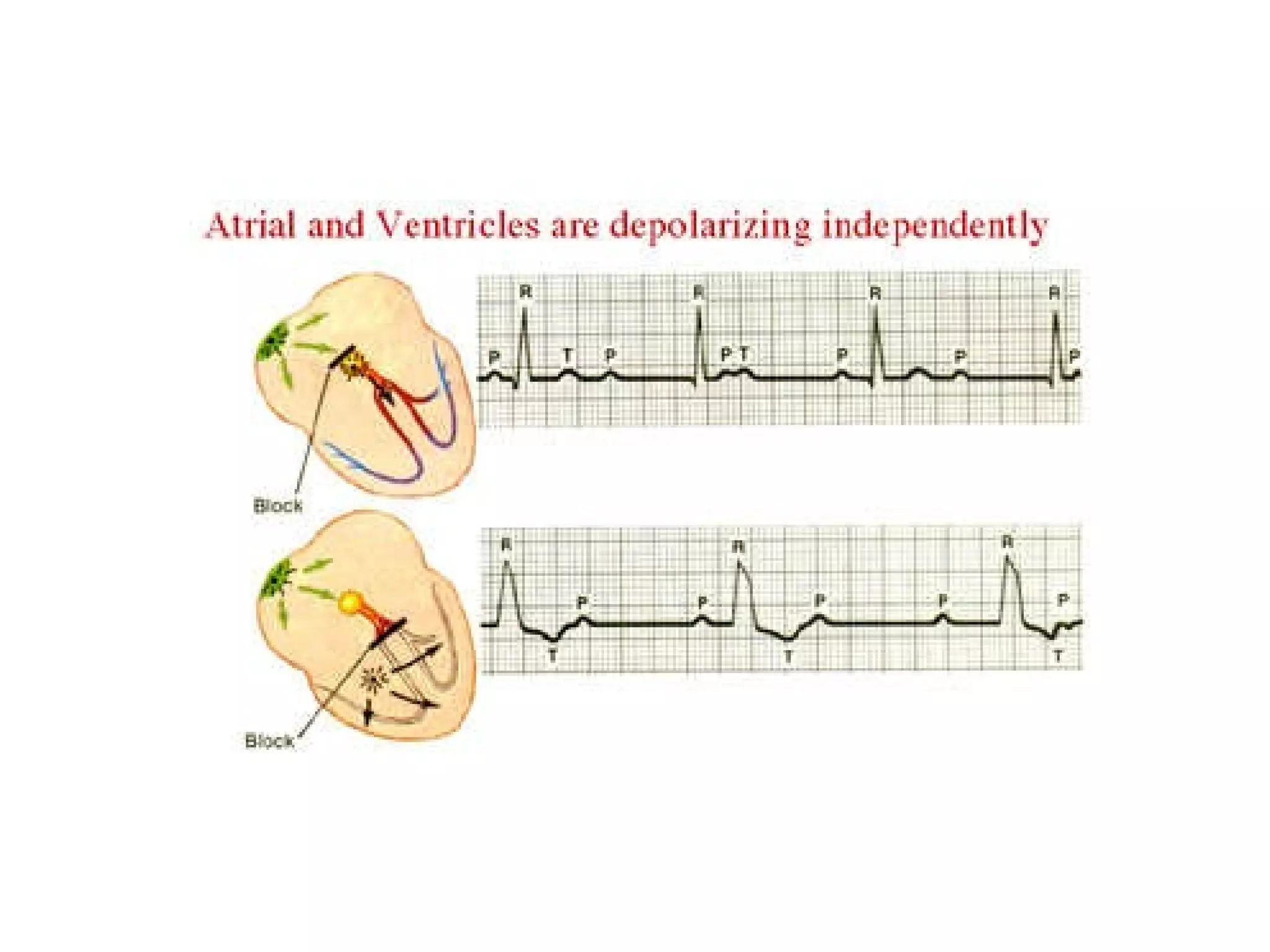
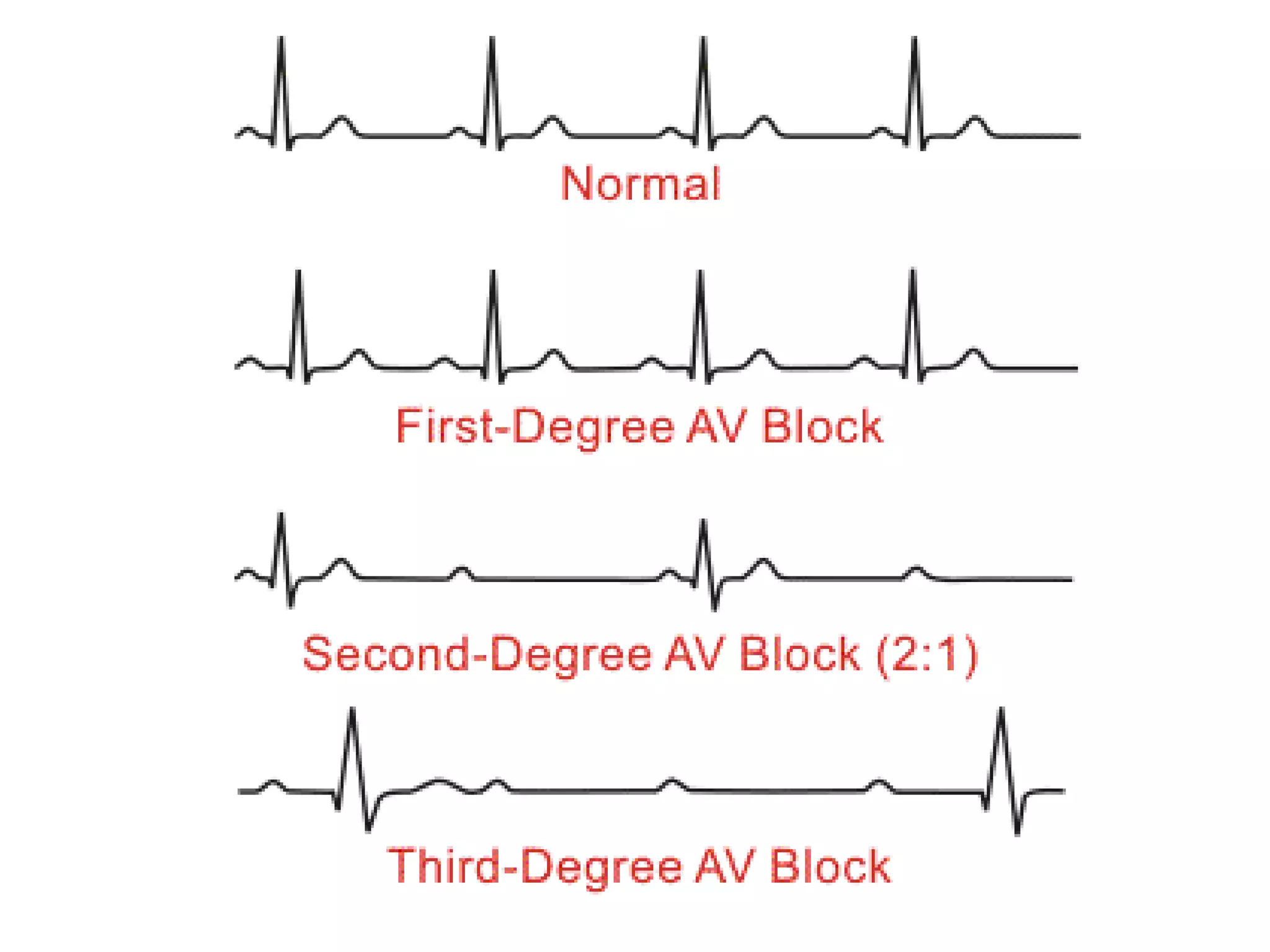
The document discusses different types of atrioventricular blocks (AV blocks), including first-, second-, and third-degree AV blocks. It defines each type of block, describes their characteristic electrocardiogram patterns including rhythm, rate, and P wave and PRI intervals. Causes of temporary and permanent AV blocks are outlined. Management of complete AV block may involve pacemaker placement depending on symptoms and heart rate.



































![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)