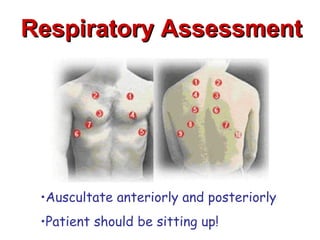
This document discusses the importance of comprehensive cardiac assessment beyond just listening to heart sounds. It emphasizes that nurses are responsible for around-the-clock surveillance of patients and should act as detectives to identify any abnormalities. The document provides guidance on key components of cardiac assessment including taking a thorough history, performing a focused physical exam, reviewing vital signs, and considering diagnostic testing based on findings.

![Blood Pressure
Blood pressure is affected by factors such as
CO [preload, contractility, afterload]; distension
of the arteries; and the volume, velocity, and
viscosity of the blood (Smeltzer et al, 2008, p. 799)
Blood pressure is an indicator of adequate or
inadequate perfusion
Inadequate perfusion may be a result of high or
low blood pressures](https://image.slidesharecdn.com/cardiacassessment-120319175201-phpapp01/85/Cardiac-Assessment-BMH-Tele-26-320.jpg)























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















