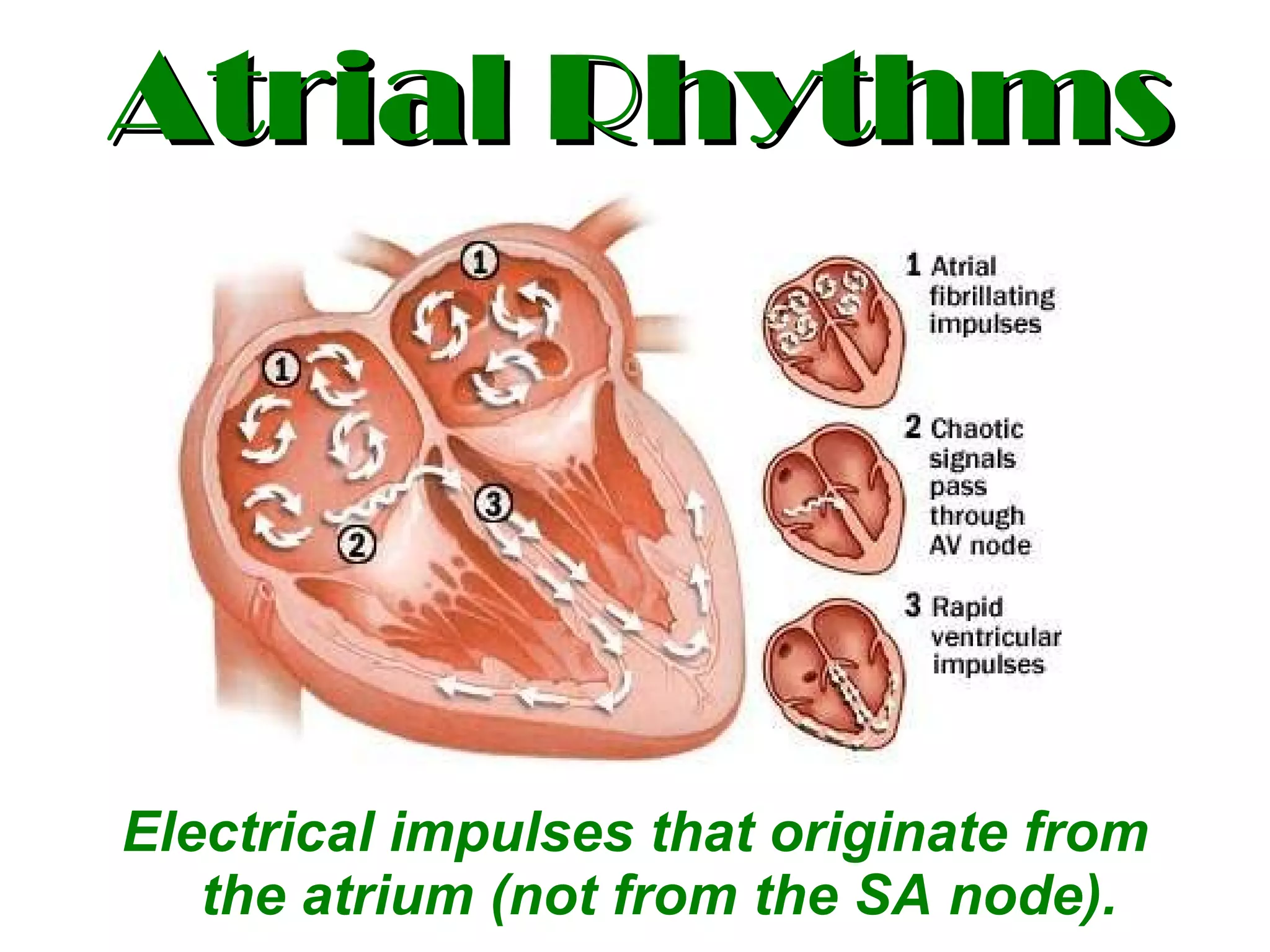
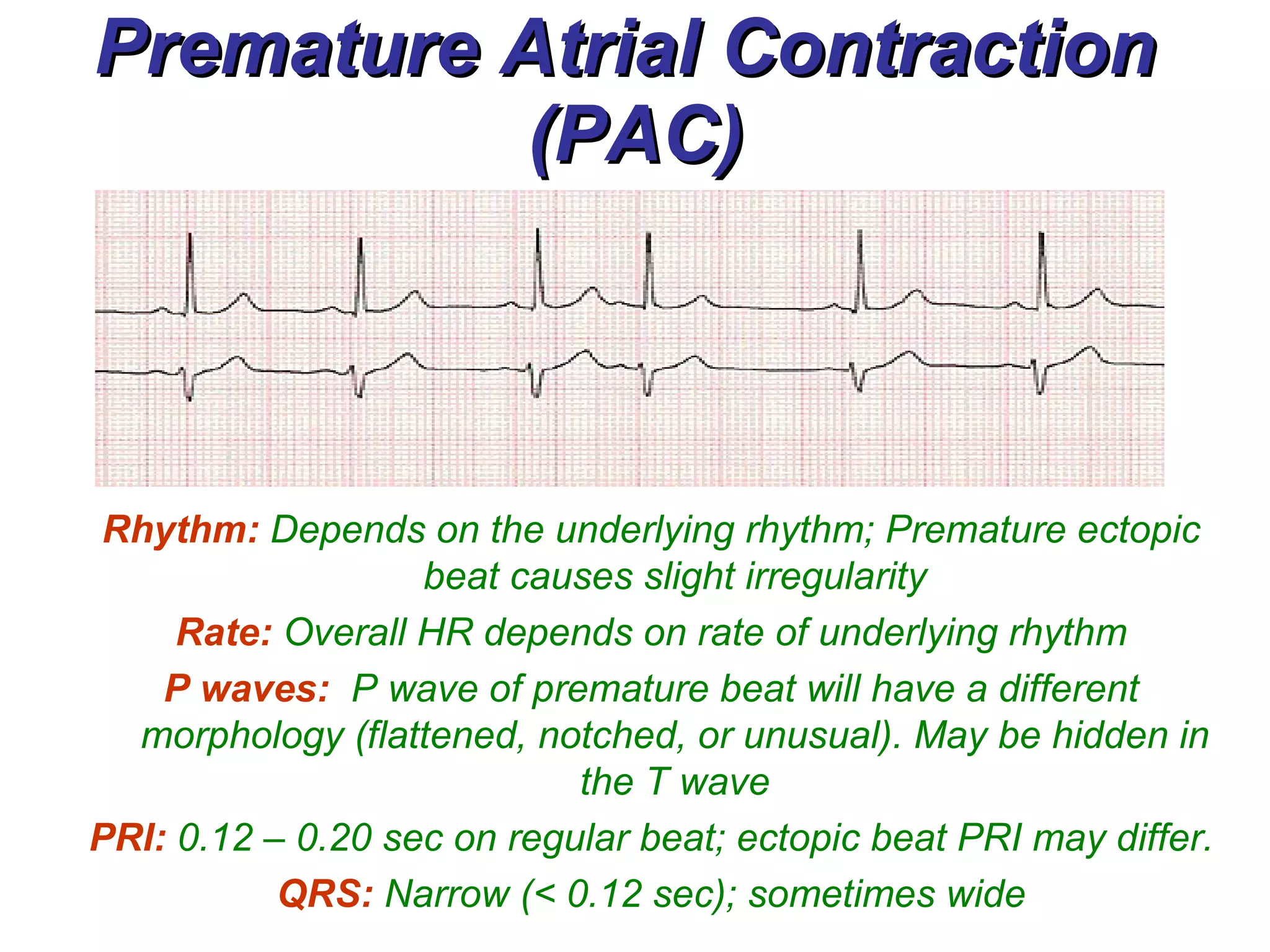
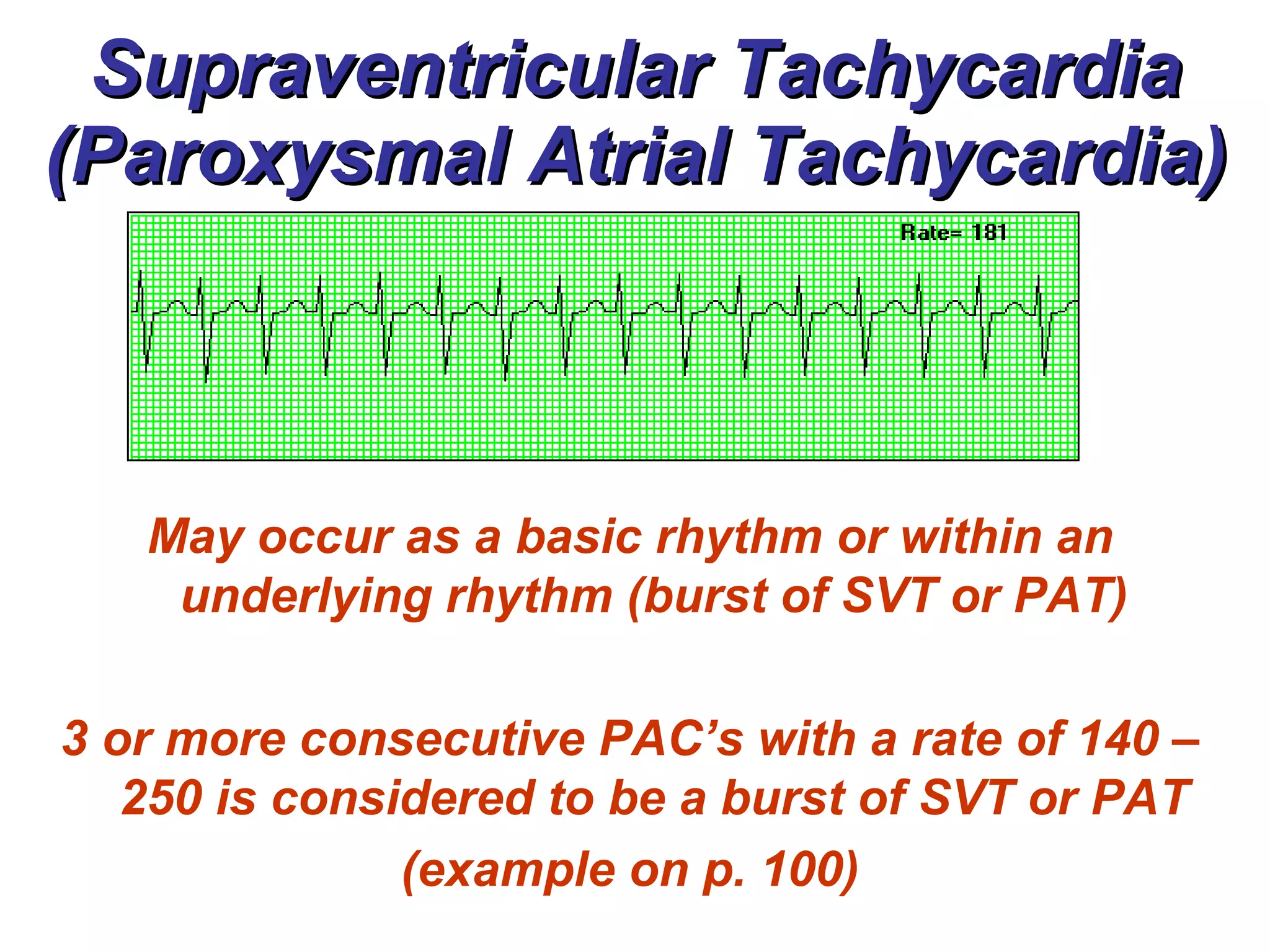
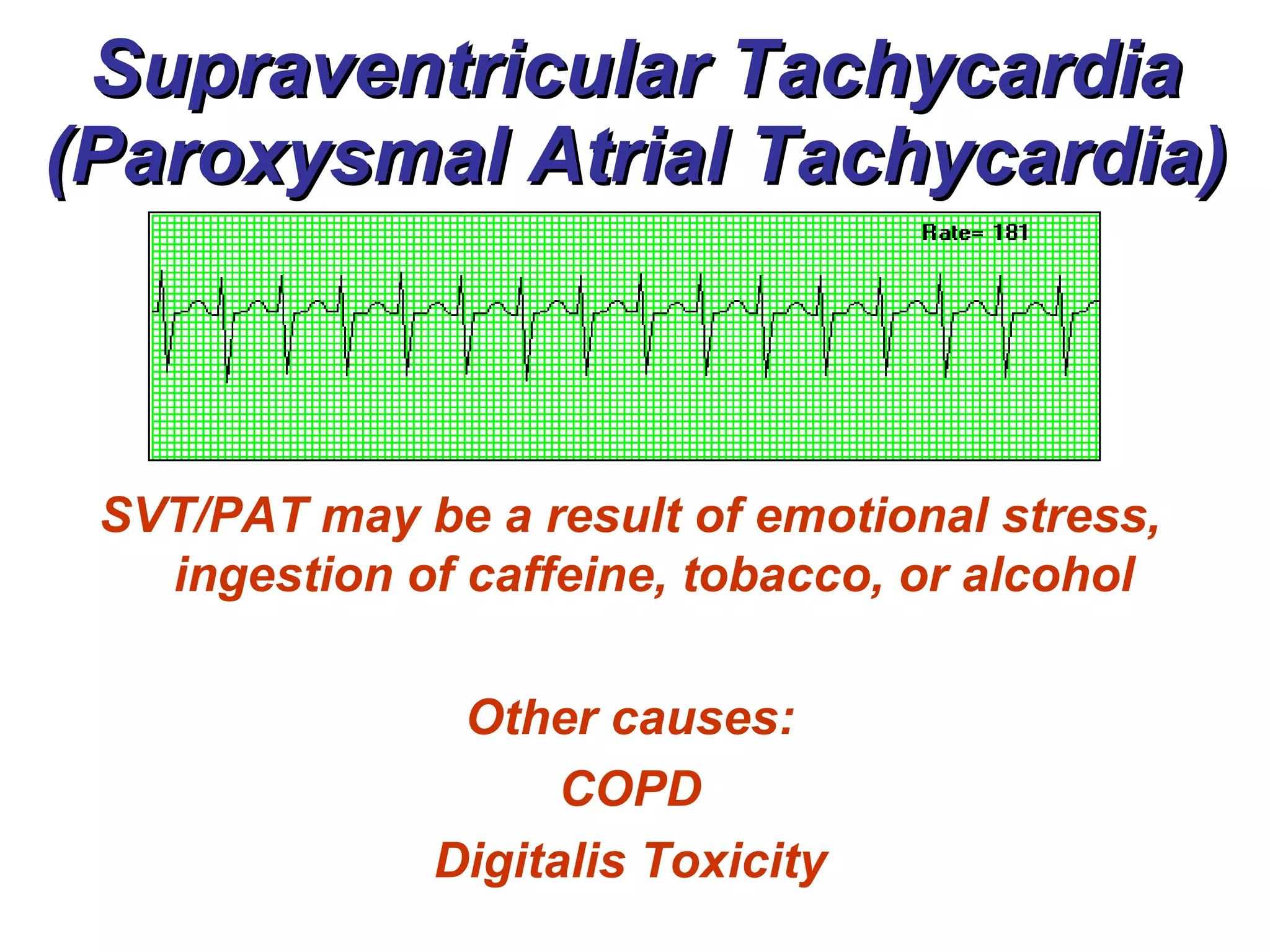
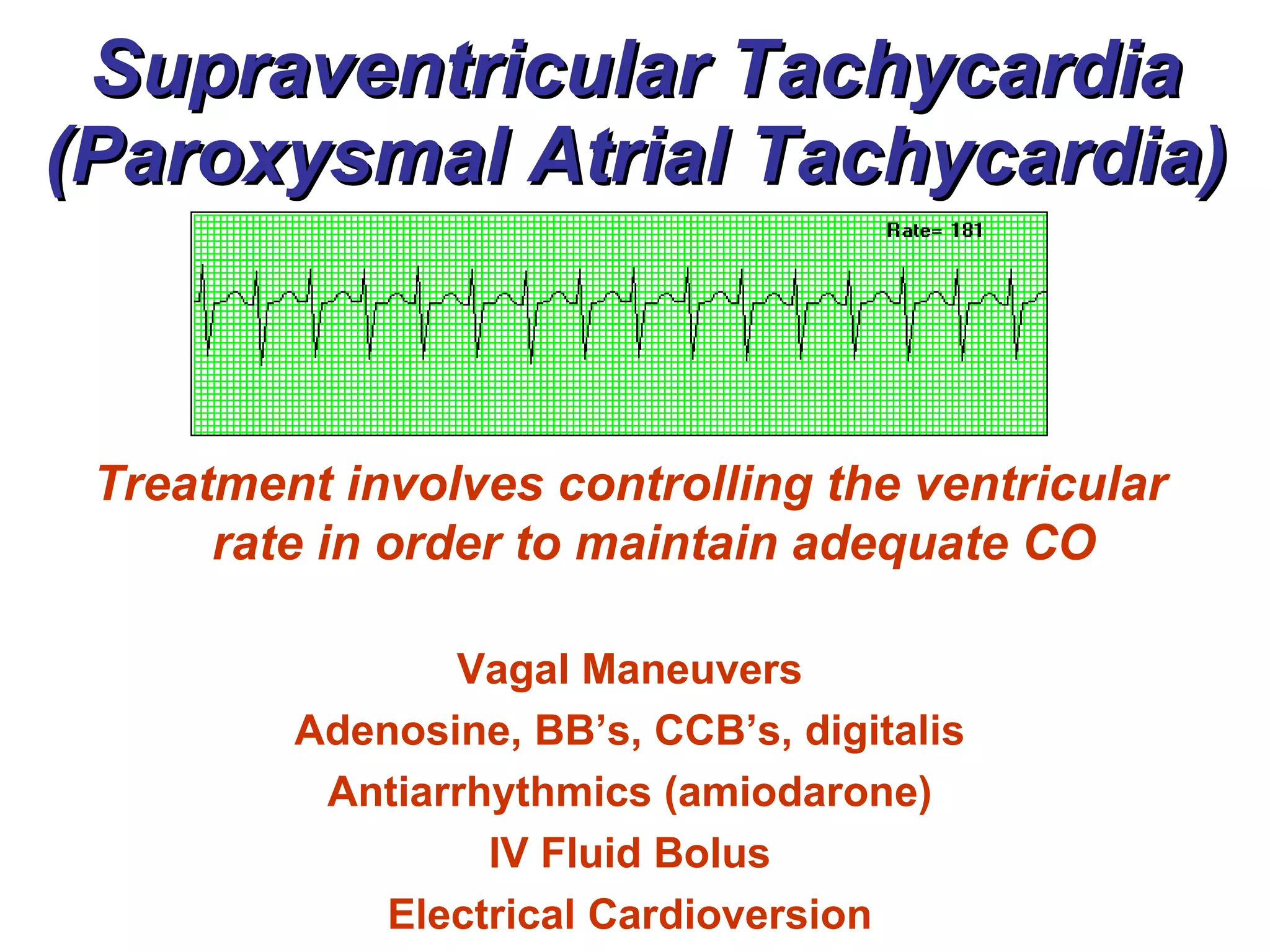
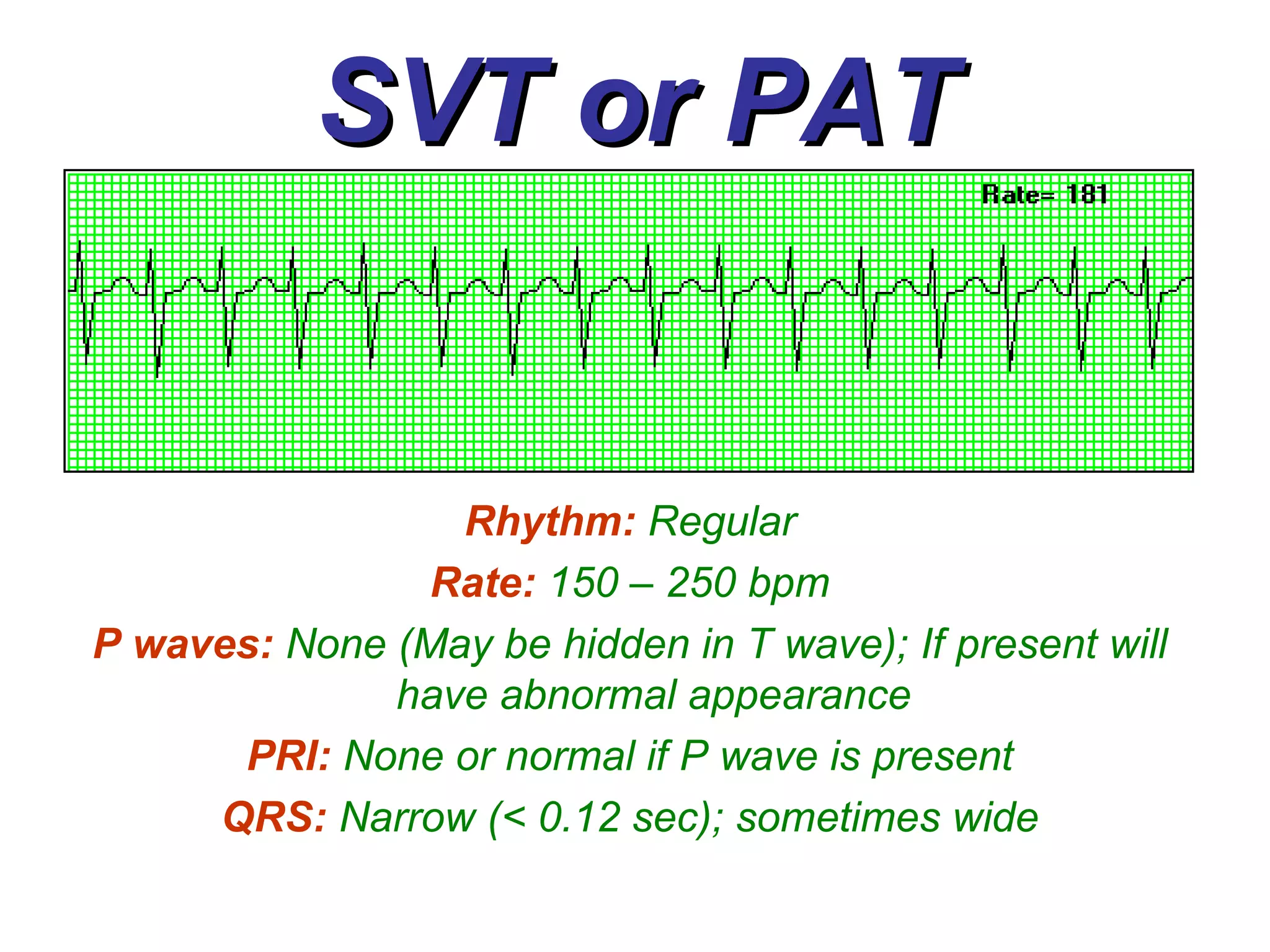
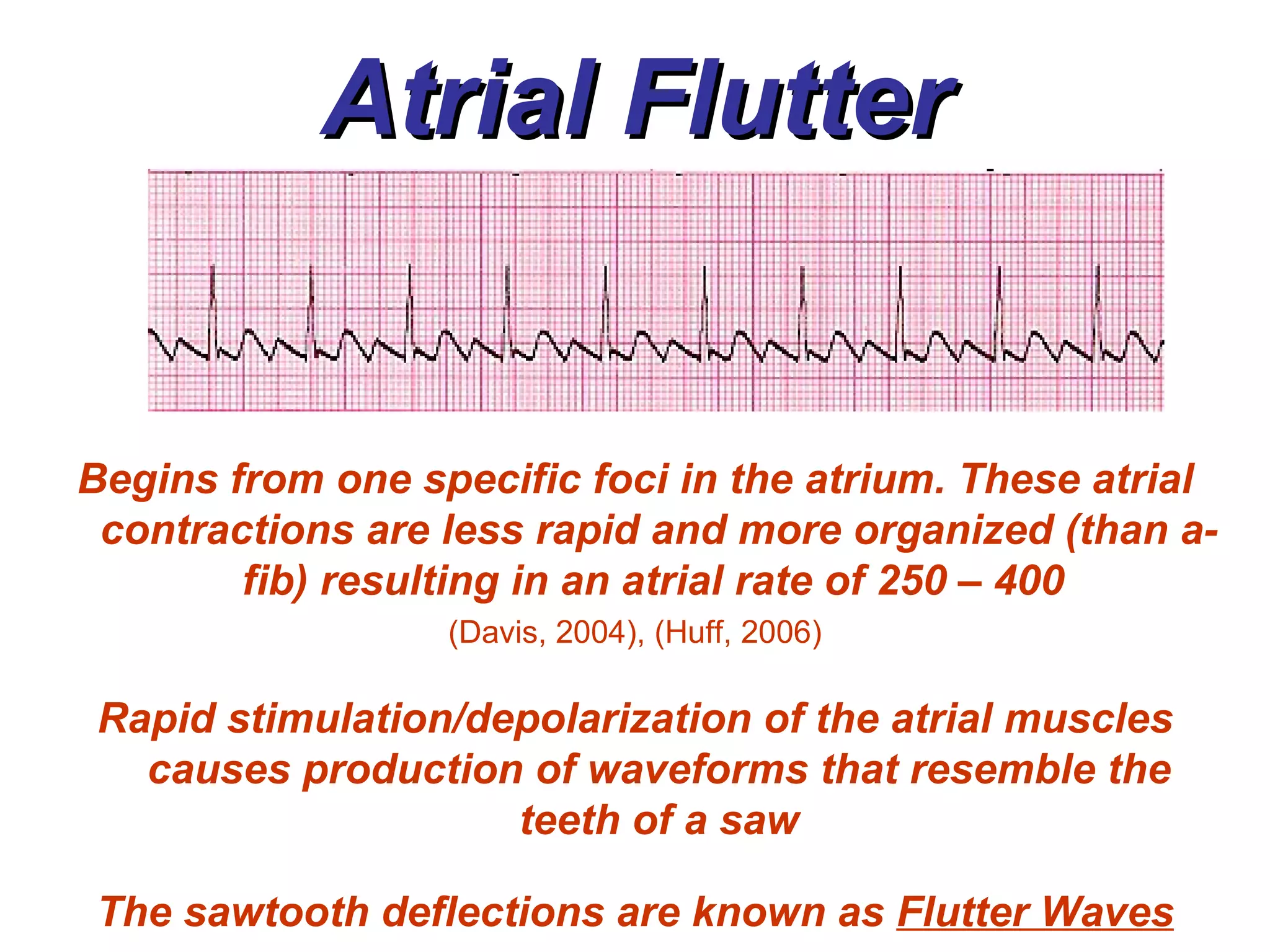
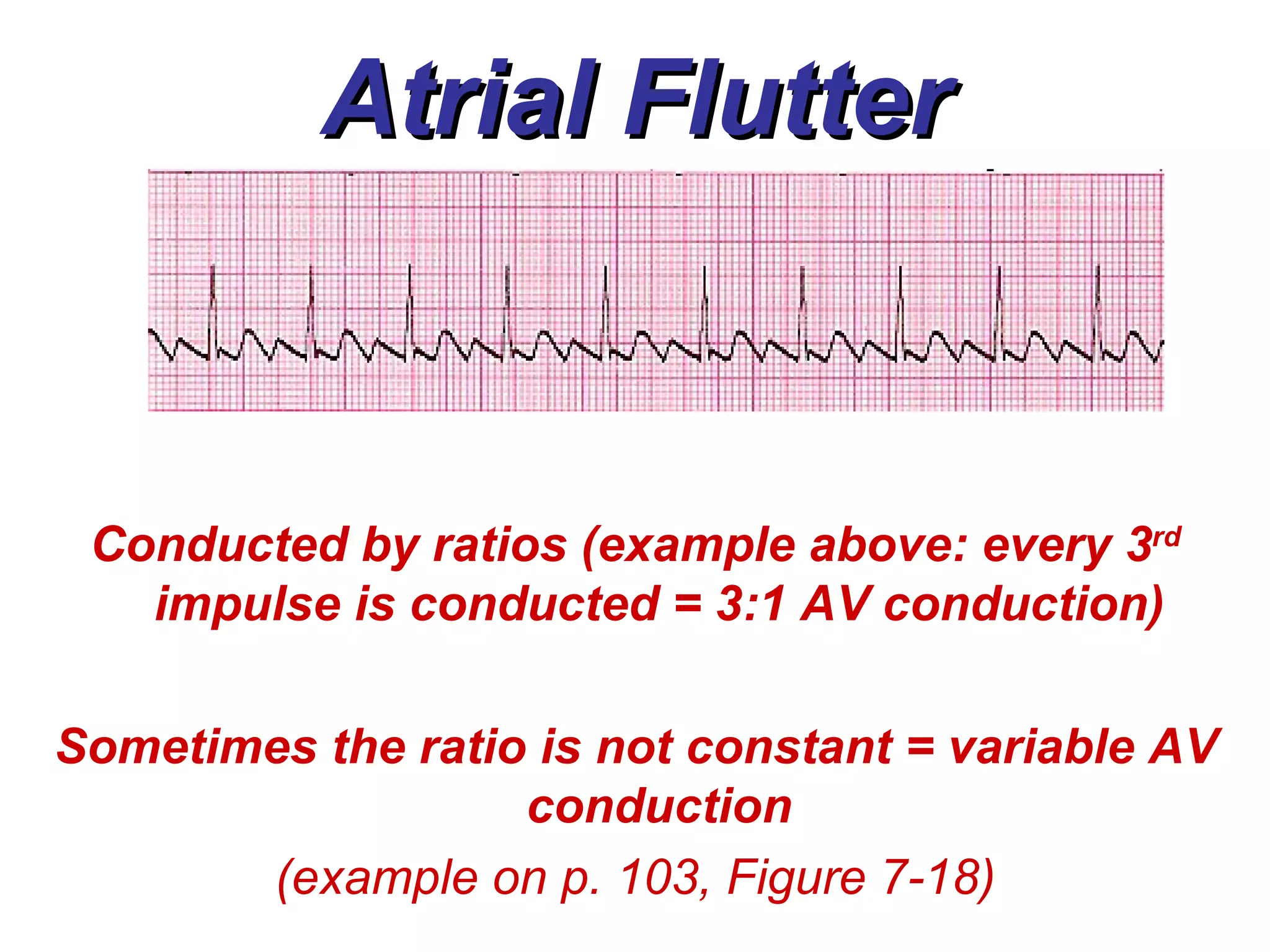
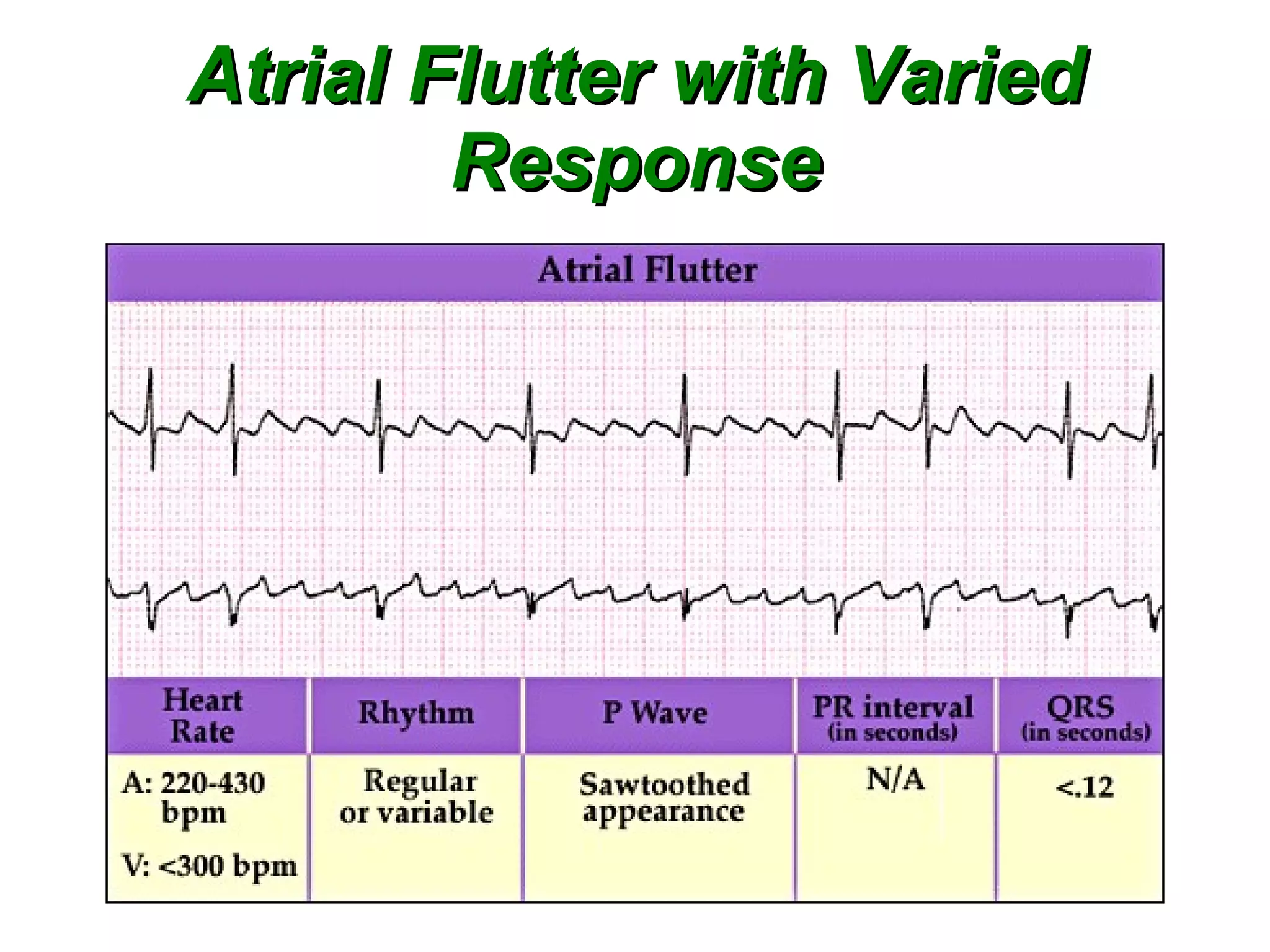
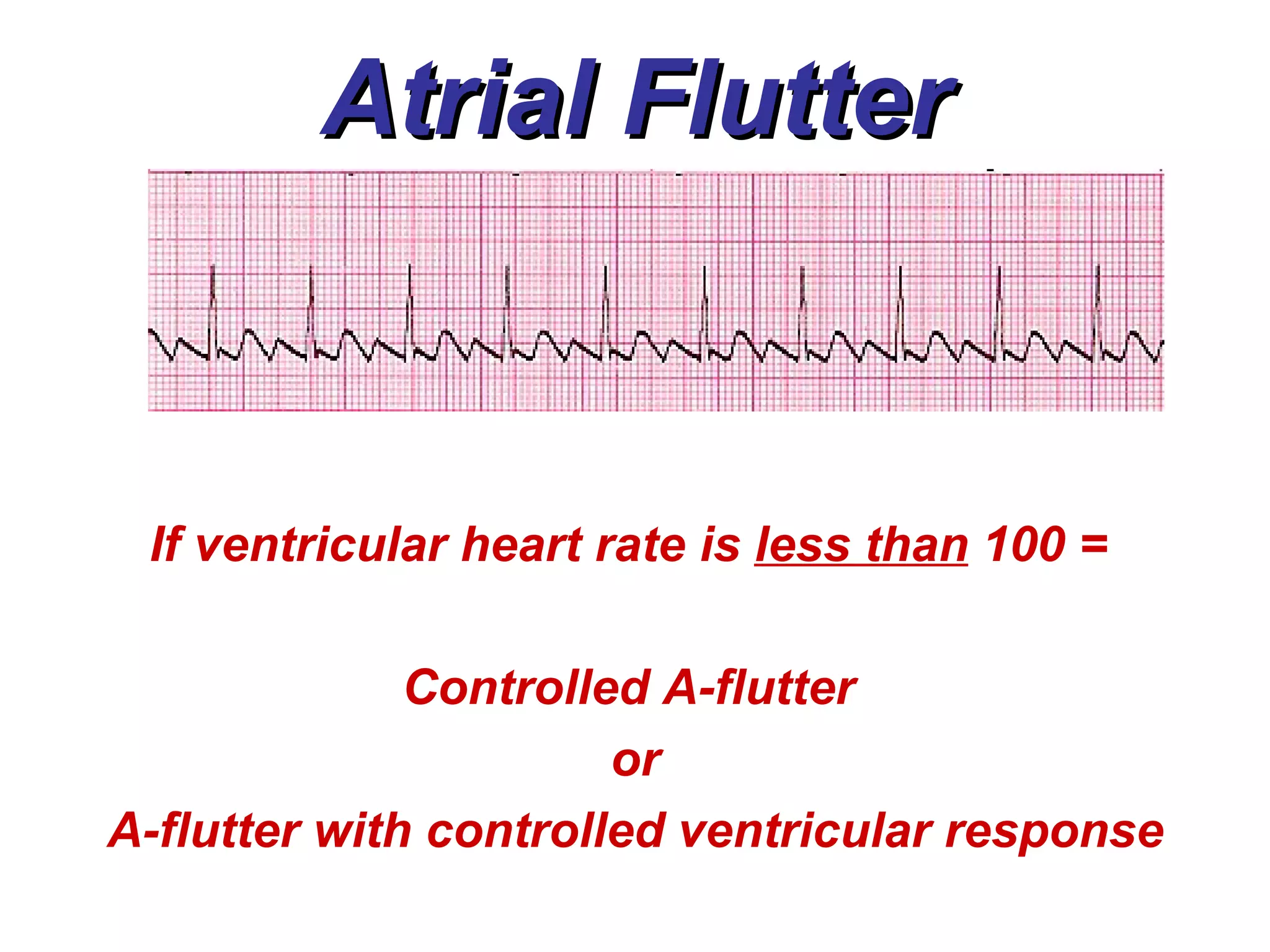
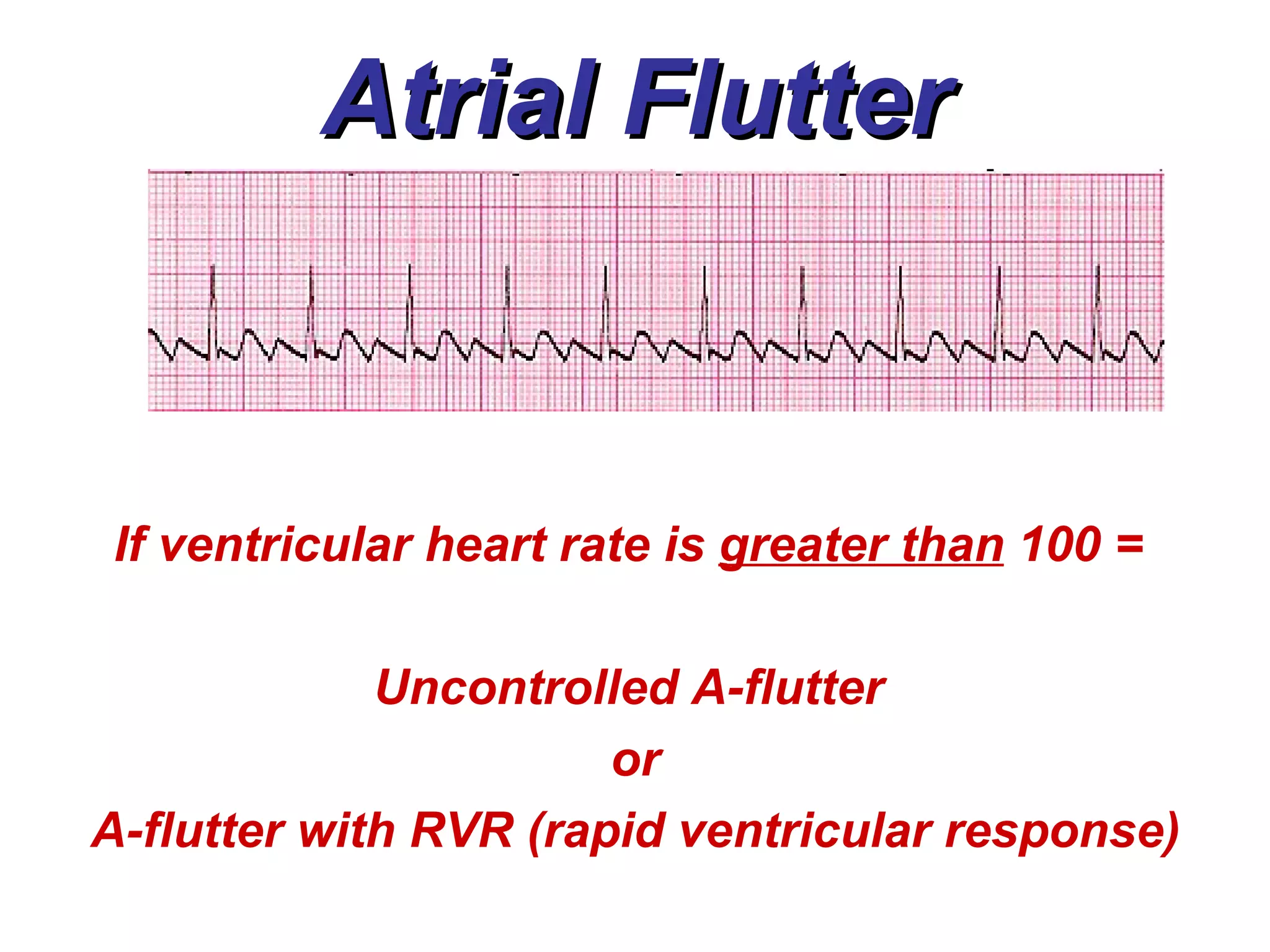
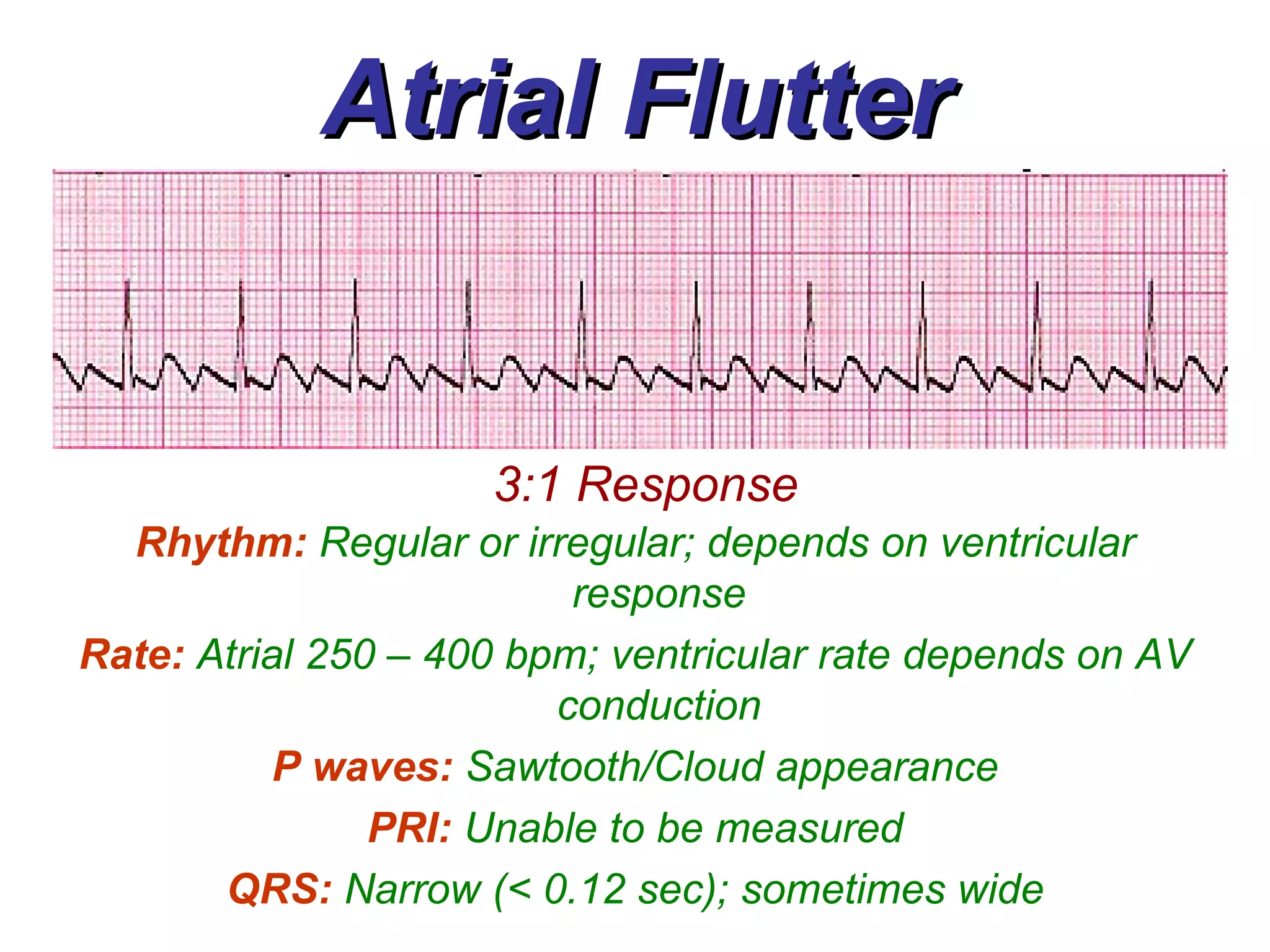
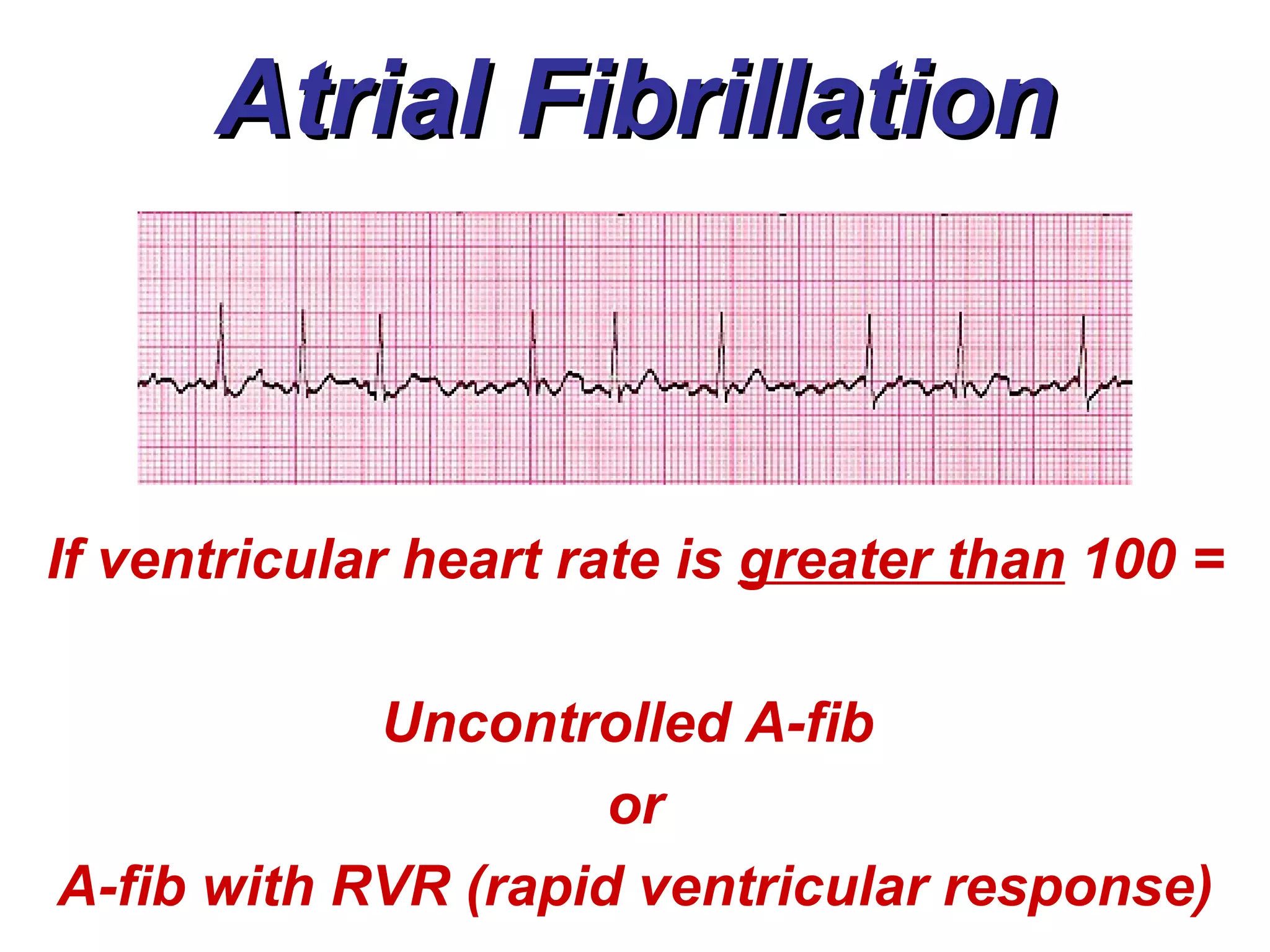
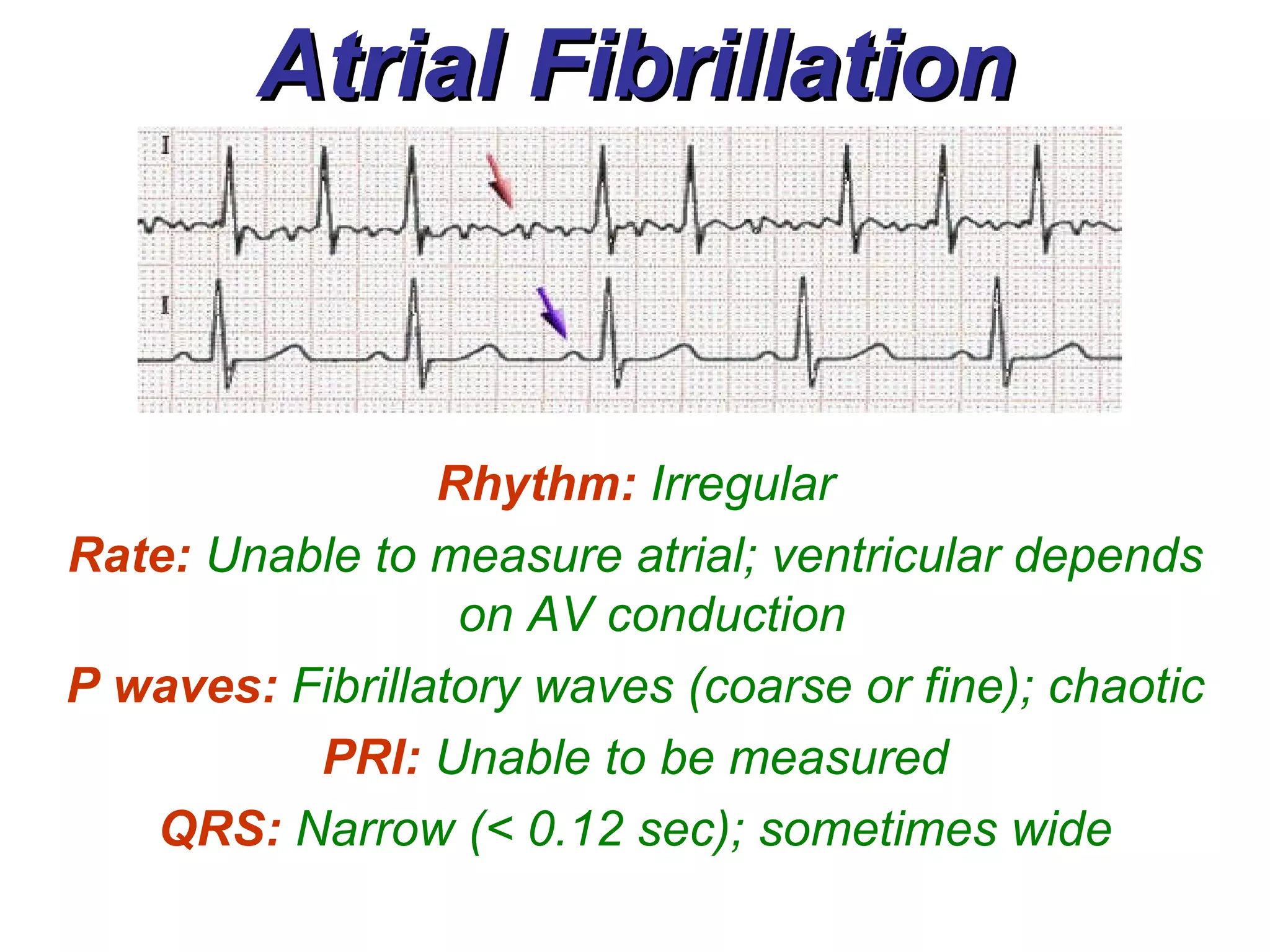
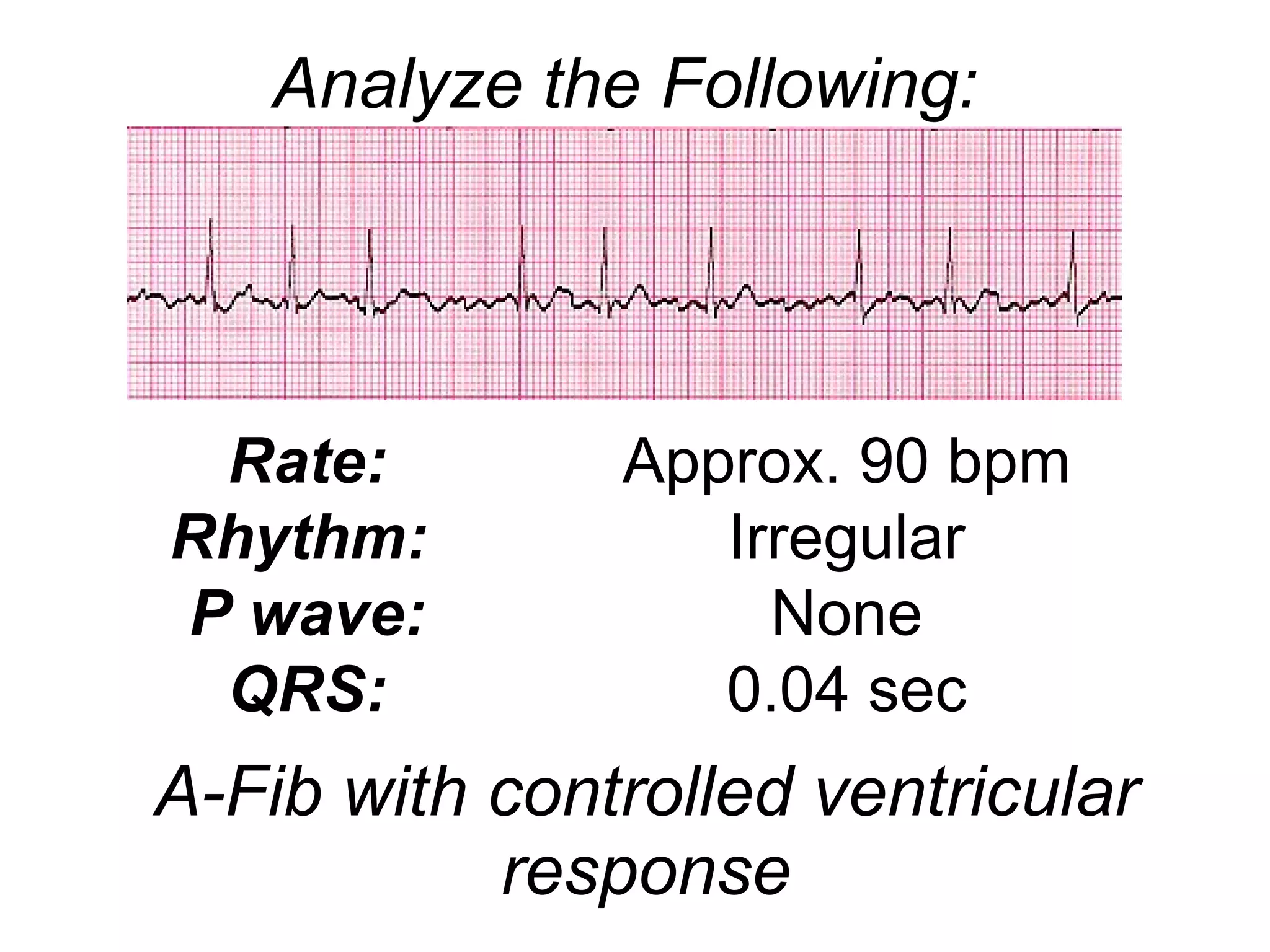
The document provides information about various types of atrial rhythms, including wandering atrial pacemaker rhythm, premature atrial contractions, supraventricular tachycardia, atrial flutter, and atrial fibrillation. It describes the characteristics of each rhythm such as rate, P wave morphology, causes, and treatment options.





























![Shadechapter09.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter09-150421103043-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)