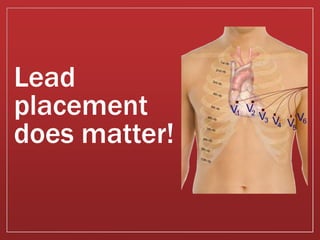
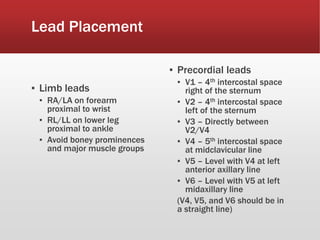
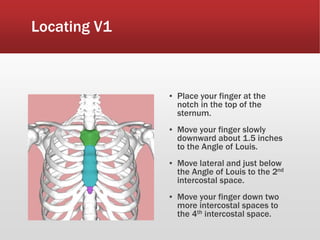
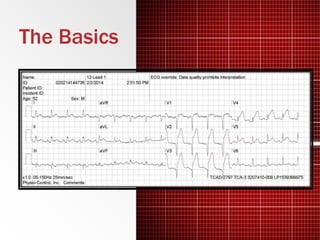
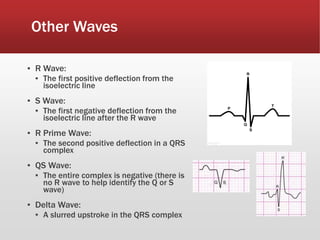
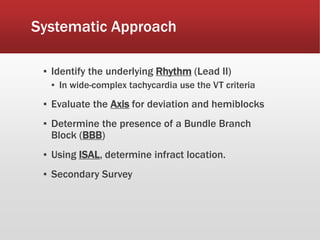
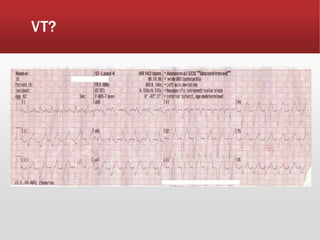
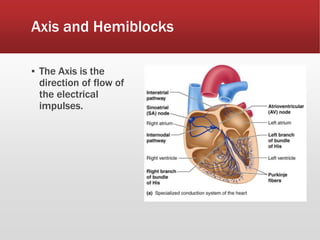
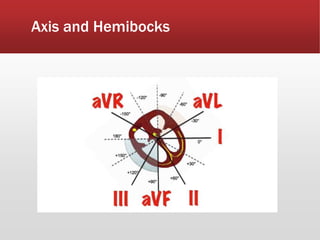
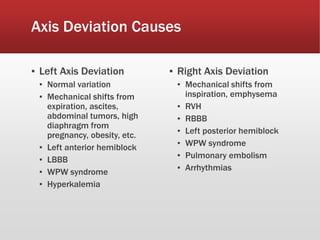
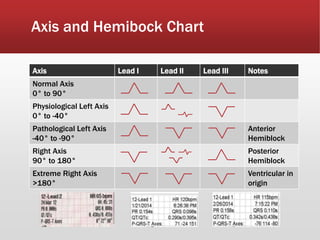
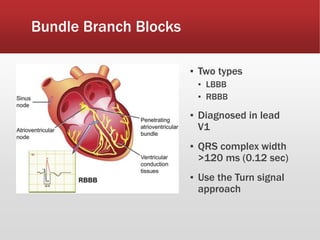
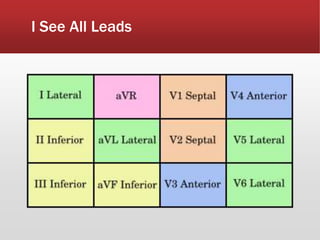
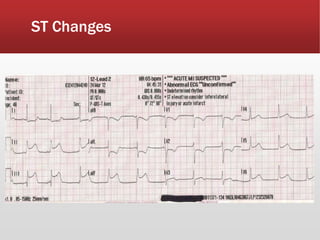
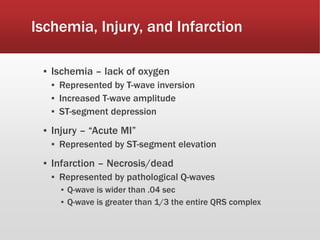
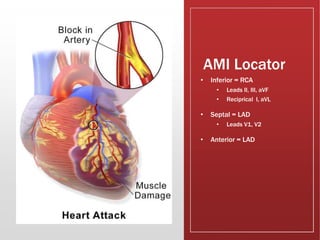
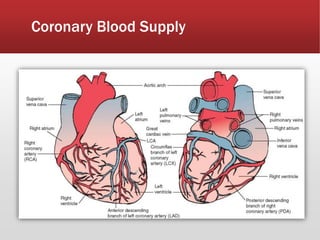
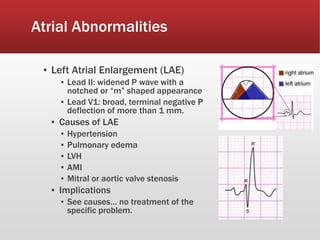
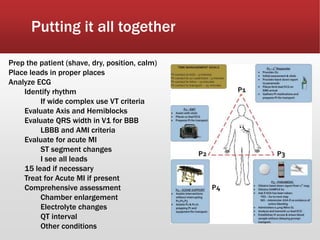
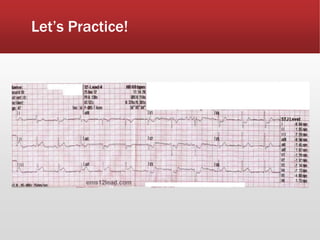
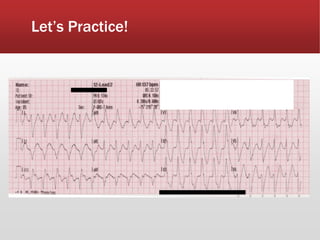
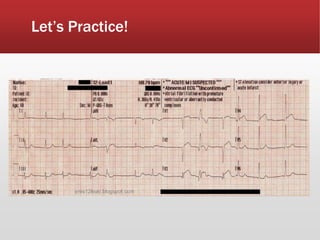
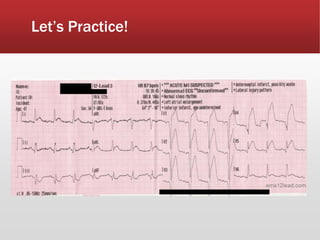
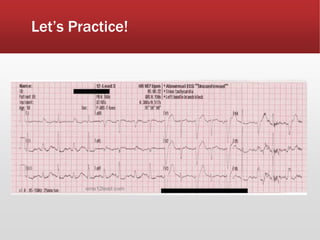
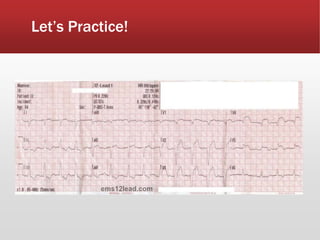
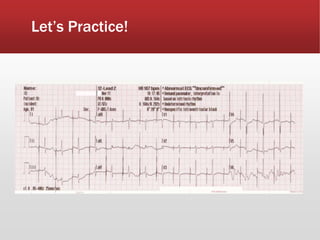
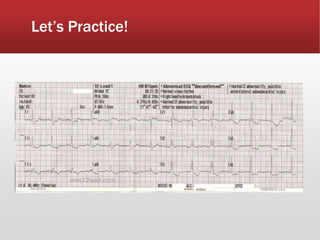
This document provides guidance on performing and interpreting multi-lead electrocardiograms (ECGs). It aims to improve patient outcomes by reducing time to percutaneous coronary intervention through early ECG acquisition and transmission. Proper lead placement is emphasized for 12- and 15-lead ECGs. A systematic approach to ECG interpretation is outlined, including identifying the underlying rhythm, assessing the axis and potential hemiblocks or bundle branch blocks, using the ISAL method to determine infarct location, and evaluating for atrial abnormalities. Key waves, intervals, and criteria for identifying ventricular tachycardia, ischemia, injury, and infarction are defined.