



































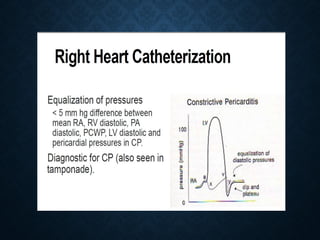









- Constrictive pericarditis results from scarring and loss of elasticity of the pericardial sac, typically due to chronic inflammation and sometimes calcification. This causes the pericardium to thicken and lose its ability to expand and contract normally. - The inelastic pericardium prevents normal filling of the heart chambers, especially in mid to late diastole. Inspiration does not decrease pressure in the left ventricle as it normally would due to the thickened pericardium isolating the heart. - Diagnosis involves physical exam findings like elevated JVP, hepatomegaly, and Kussmaul's sign combined with echocardiography findings like sept



































































