This document discusses various ventricular rhythms and arrhythmias:
- Ventricular rhythms originate from the ventricular conduction system and include bundle branch blocks, premature ventricular contractions, ventricular escape beats, idioventricular rhythms, ventricular tachycardia, and ventricular fibrillation.
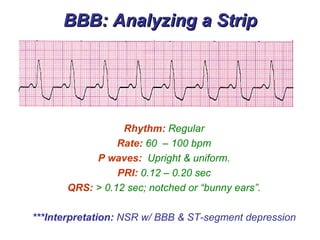
- Bundle branch blocks involve slowed conduction through one of the bundle branches, resulting in a widened QRS complex.
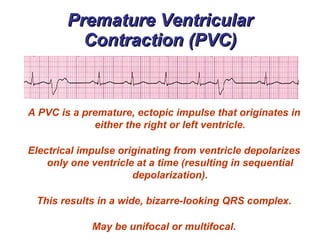
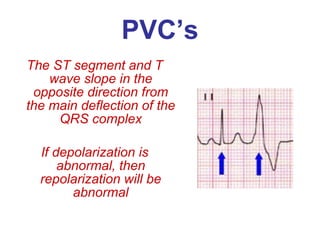
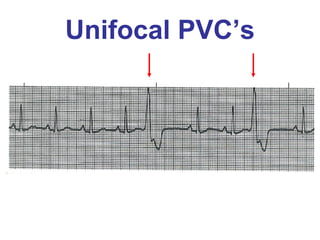
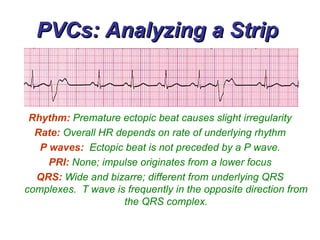
- Premature ventricular contractions originate from ectopic sites in the ventricles and cause the ventricles to depolarize sequentially, resulting in a wide, bizarre QRS complex.
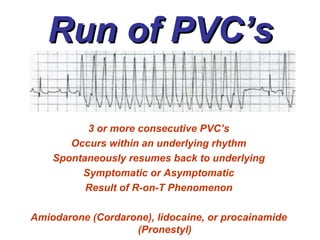
- Ventricular tachycardia is a regular, rapid rhythm originating from the ventricles that can








































































![Shadechapter14.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter14-150421104301-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)










![Shadechapter11.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter11-150421103622-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)