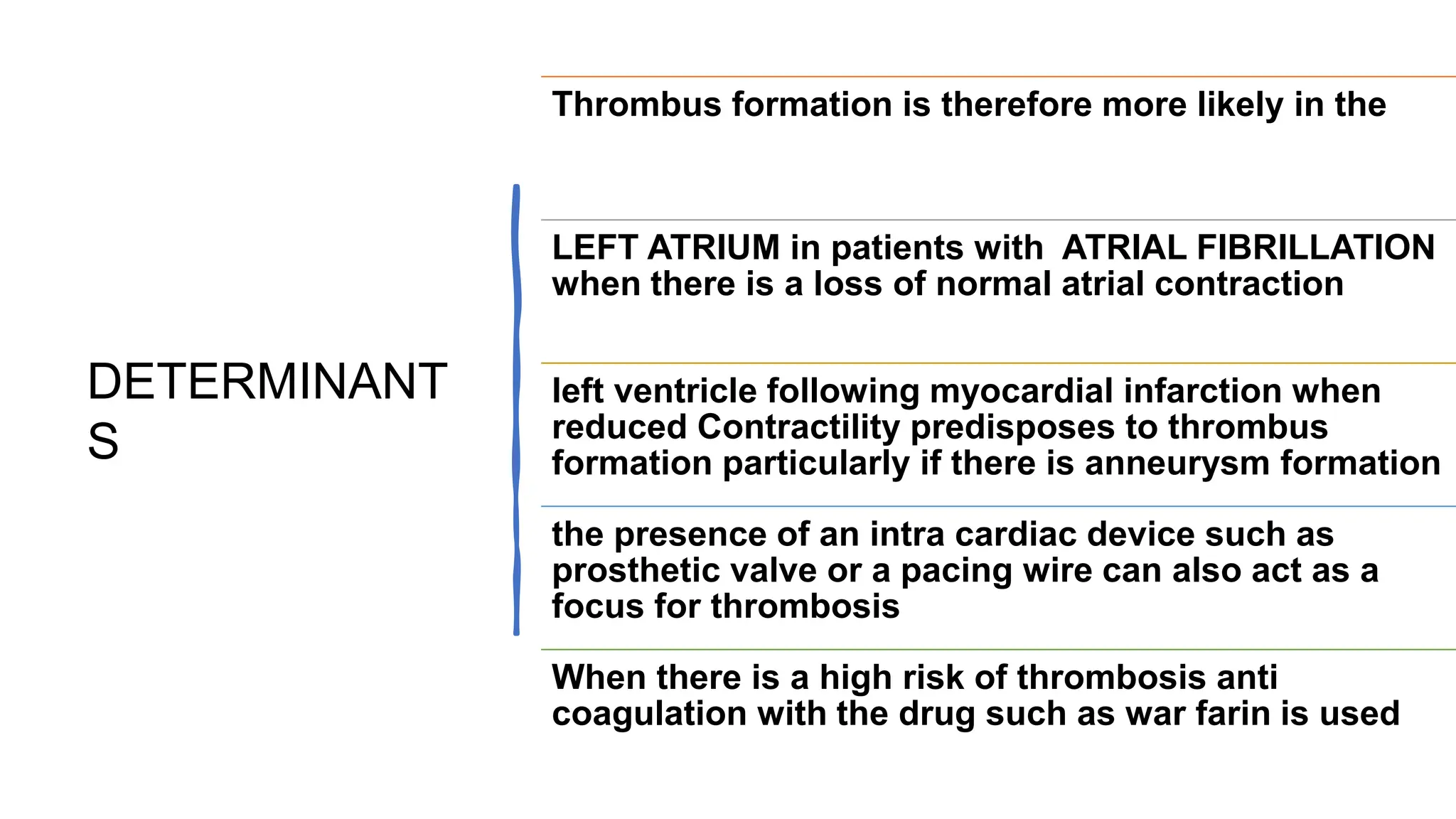
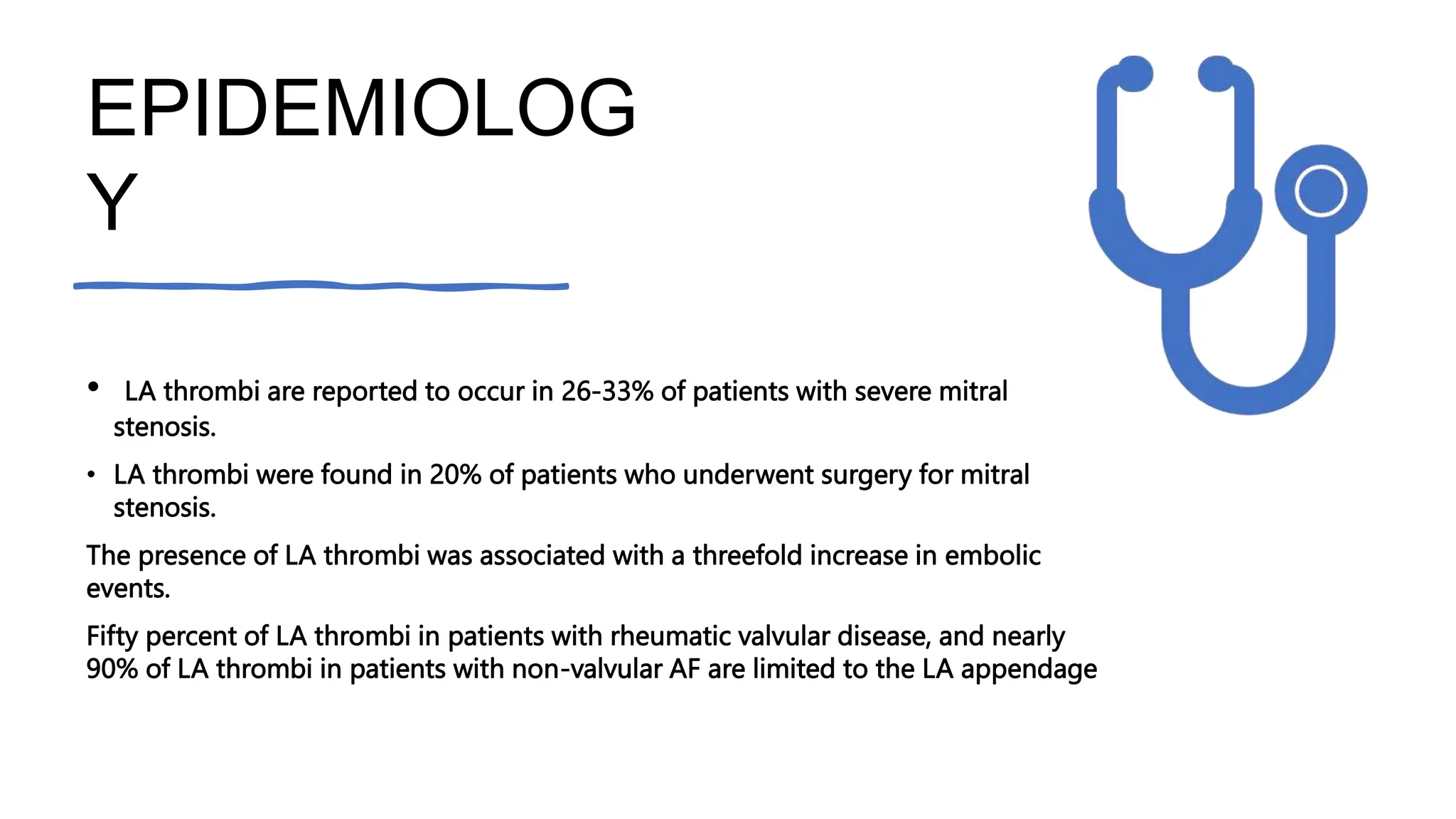
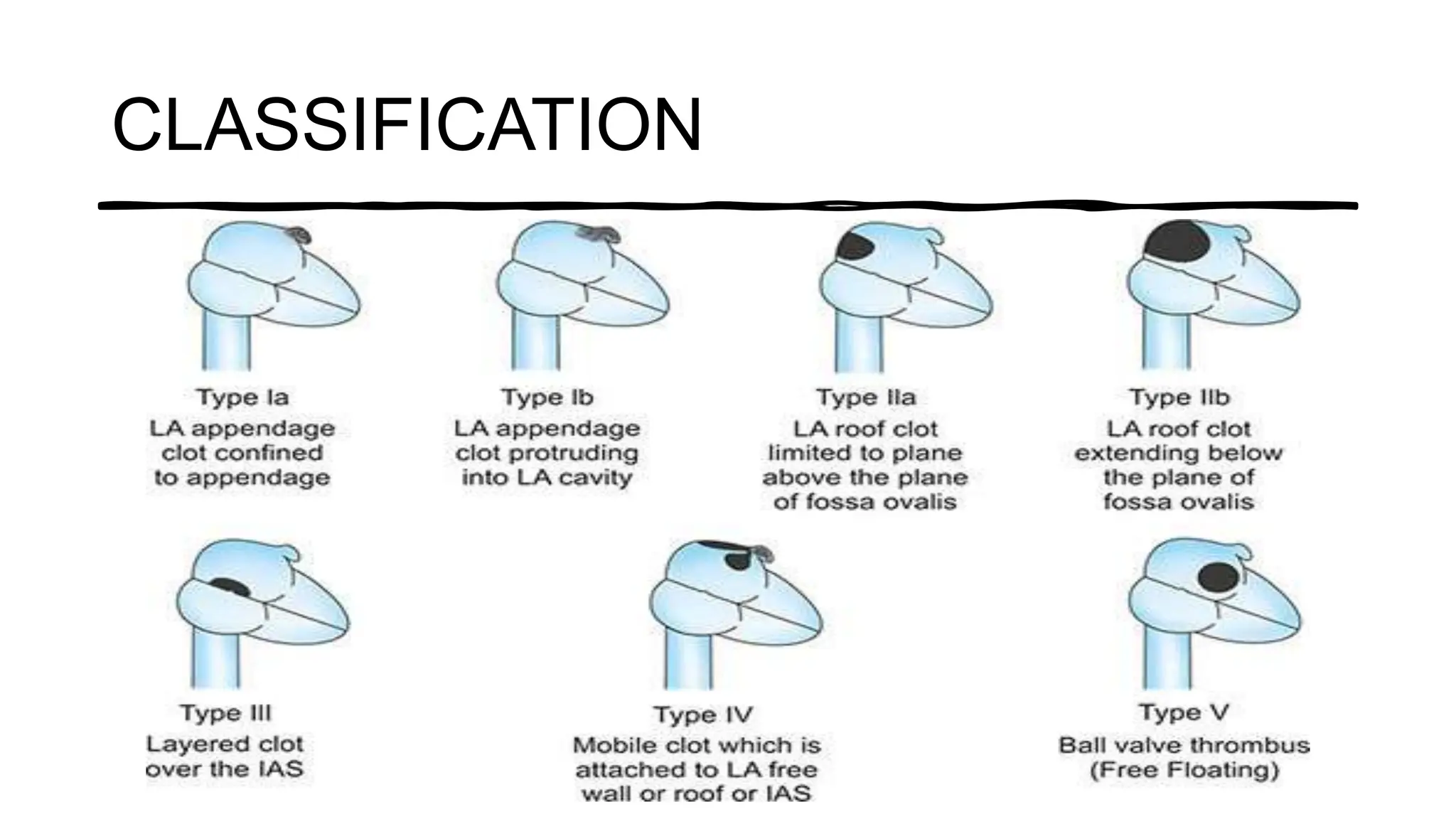
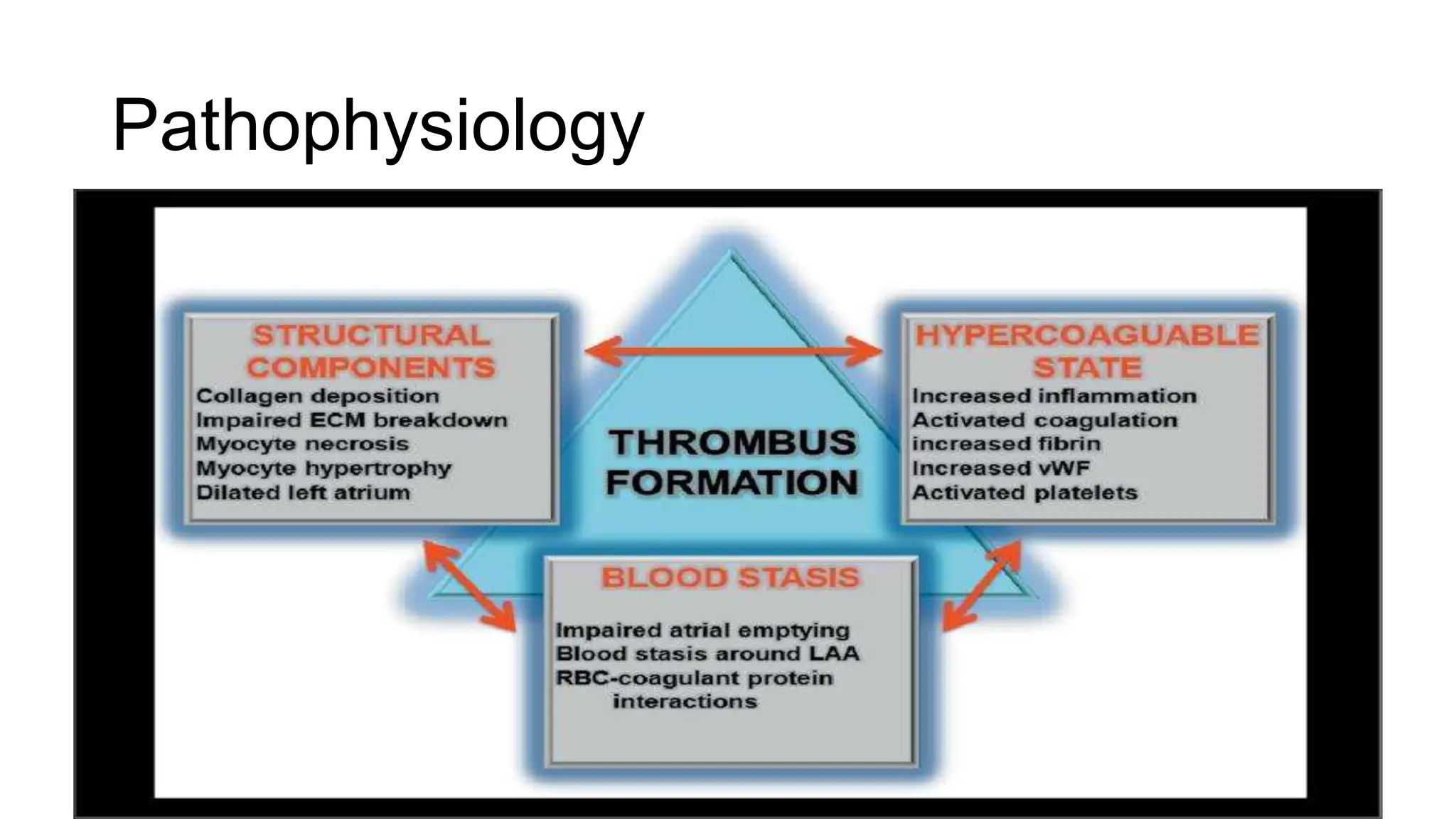
The document discusses the formation and implications of thrombus, particularly in the context of atrial fibrillation and mitral stenosis. It details the risk factors, classification, and diagnostic modalities such as echocardiography for assessing left atrial thrombi. Key epidemiological findings highlight a significant prevalence of thromboembolic complications in patients with rheumatic mitral stenosis, emphasizing the left atrium and appendage as critical sites for clot formation.






































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













