Downloaded 475 times
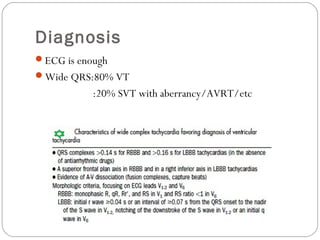
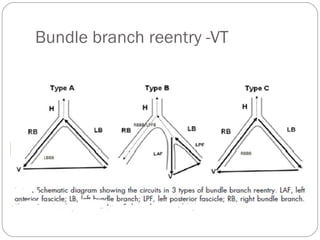
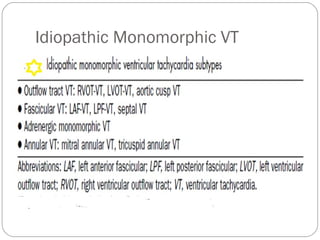
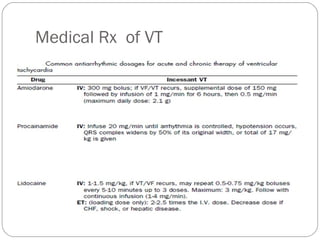
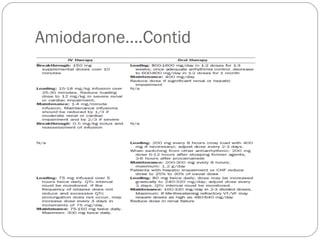
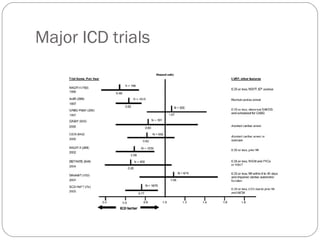
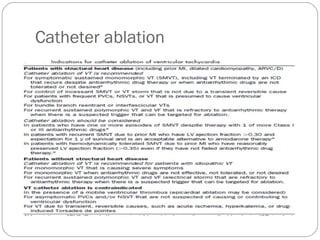

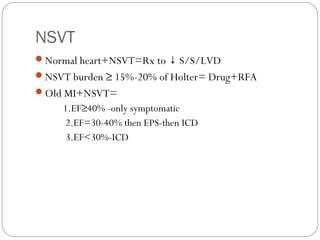

Ventricular tachycardia (VT) is an arrhythmia originating in the ventricles with a heart rate over 100 beats per minute and wide QRS complexes of at least 120 ms. VT can be either idiopathic or structural, sustained or non-sustained, and monomorphic or polymorphic. The ECG can diagnose VT based on the wide QRS complexes. VT has subtypes including bundle branch reentry VT and idiopathic monomorphic VT. Treatment options include medical therapies like amiodarone, implantable cardioverter defibrillators based on major trials, and catheter ablation.























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




