Downloaded 1,193 times




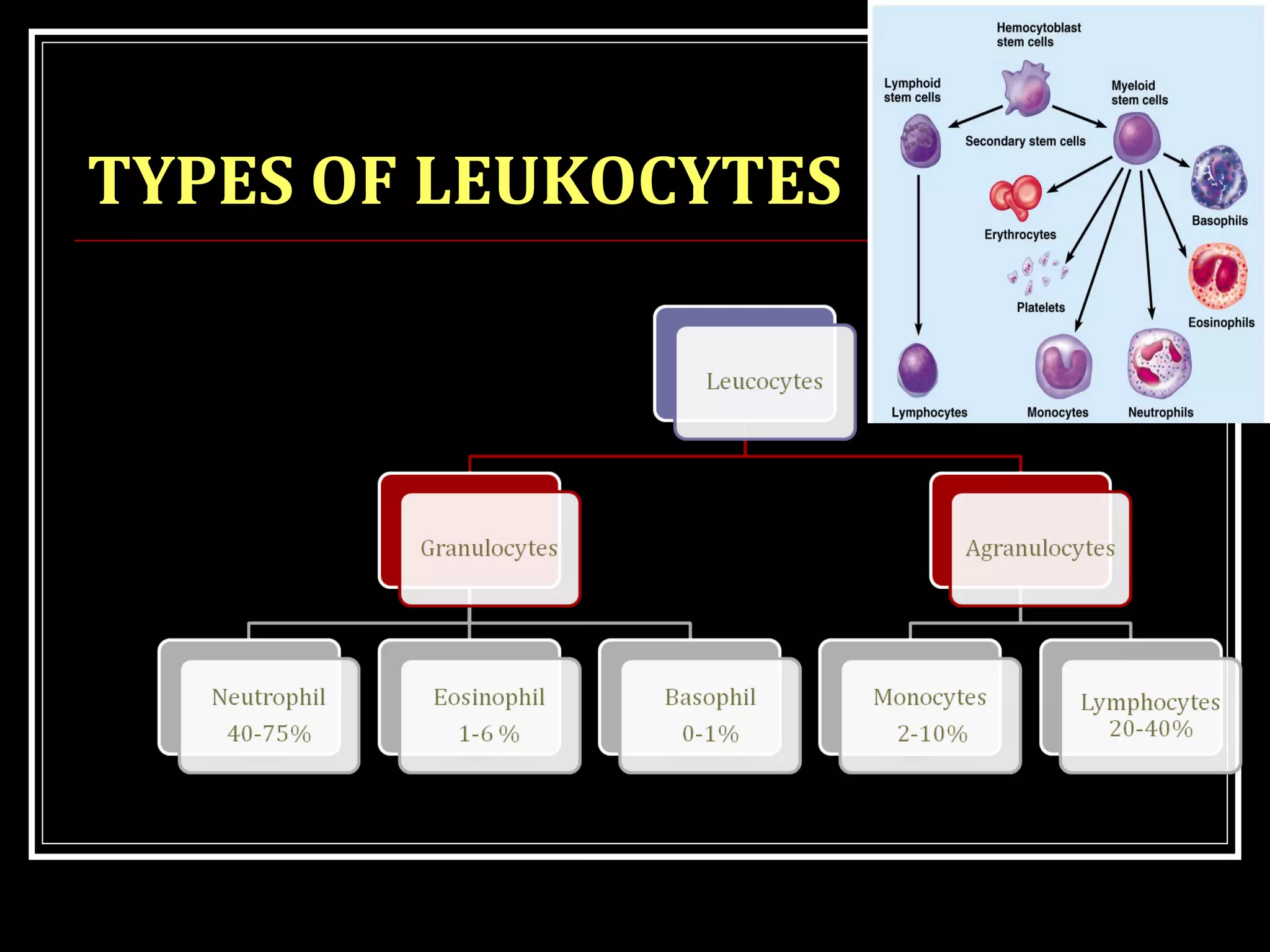

















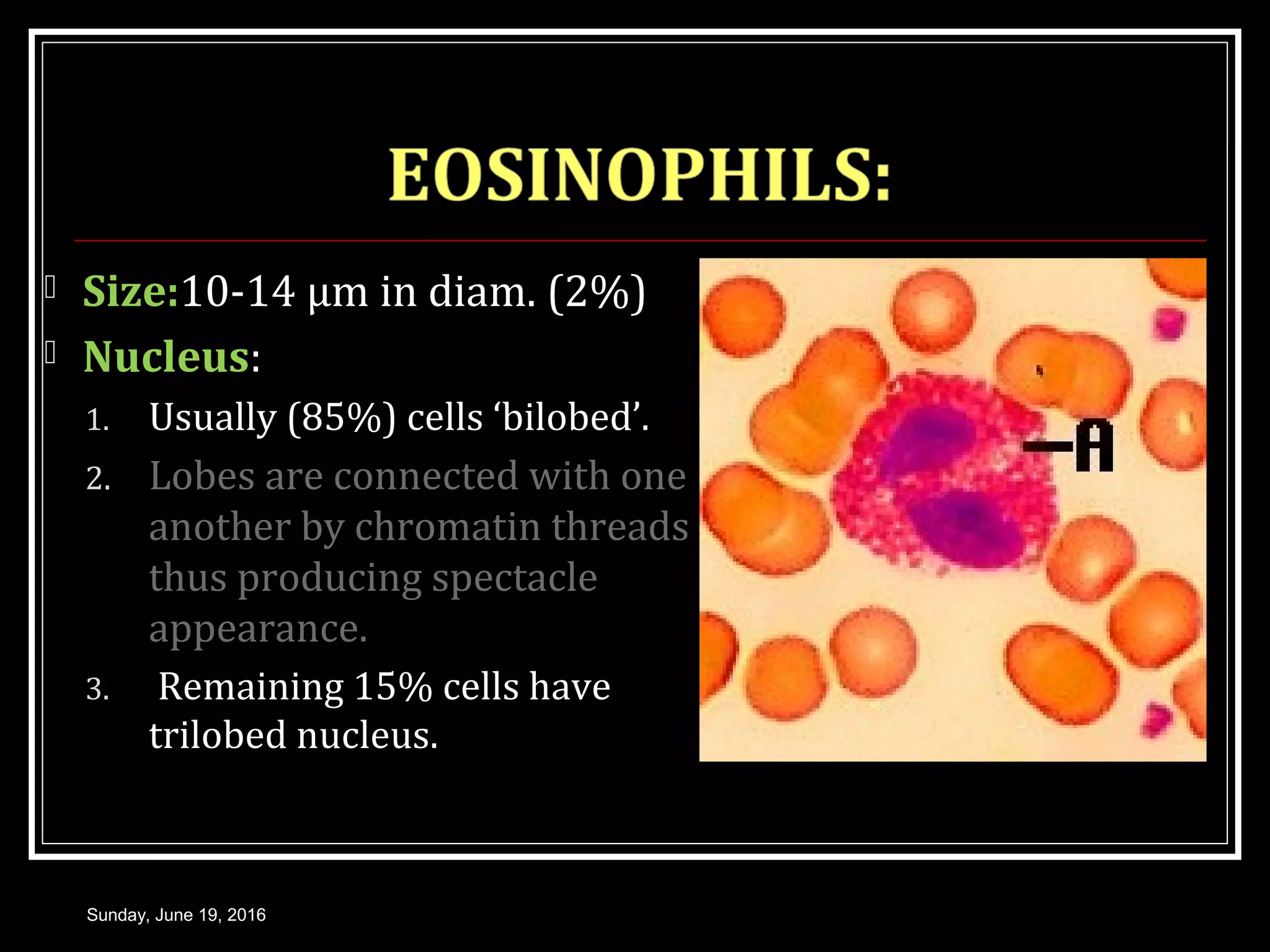




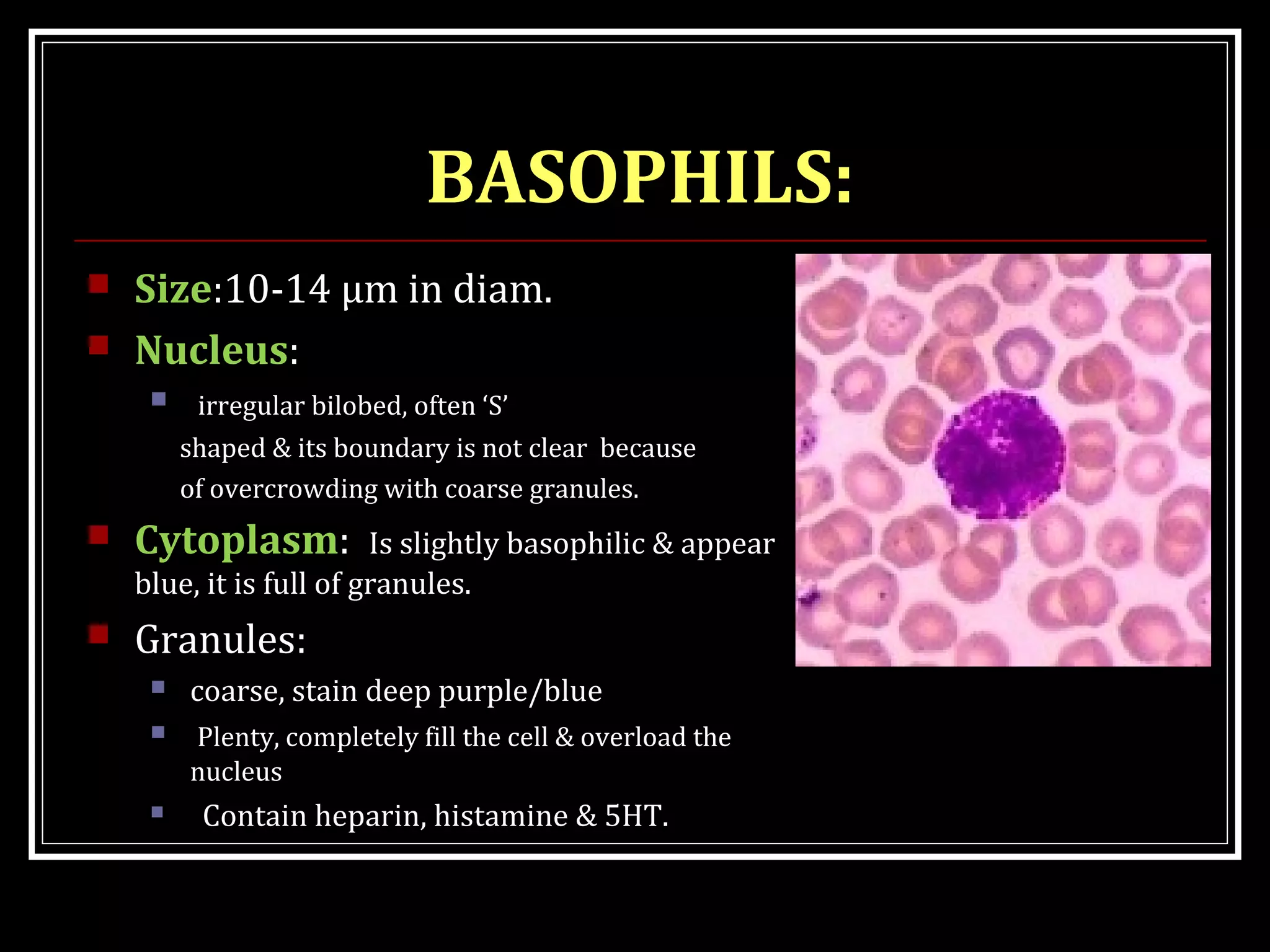













This document provides information about white blood cells (leukocytes): - It describes the main types of leukocytes - granulocytes (neutrophils, eosinophils, basophils) and agranulocytes (lymphocytes, monocytes). It details their morphology, counts, functions and factors that cause their levels to vary. - The formation (leukopoiesis), regulation and lifespan of white blood cells is explained. Key processes like phagocytosis, respiratory burst and neutrophil recruitment are summarized. - Specific details are given about each type of leukocyte - their size, nuclear morphology, cytoplasmic granules, functions and causes of increased/decreased counts.






![White blood cells [wbc]](https://cdn.slidesharecdn.com/ss_thumbnails/whitebloodcellswbc-180530054405-thumbnail.jpg?width=640&height=640&fit=bounds)