Downloaded 1,478 times



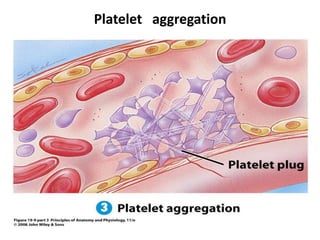






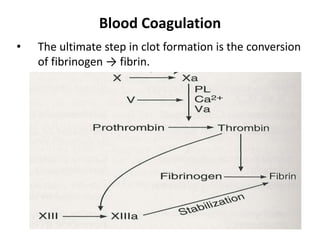
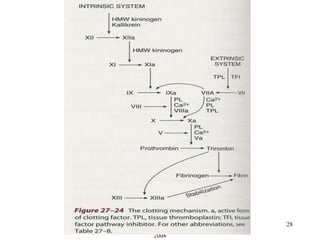









This document summarizes blood coagulation and hemostasis. It discusses platelets, the platelet plug formation process, and the intrinsic and extrinsic pathways of blood coagulation. Disorders of coagulation covered include hemophilia A/B/C, von Willebrand disease, and purpura. Tests of hemostatic function like bleeding time, clotting time, and prothrombin time are also outlined. Anticoagulants like heparin and warfarin are briefly described.