Downloaded 1,507 times

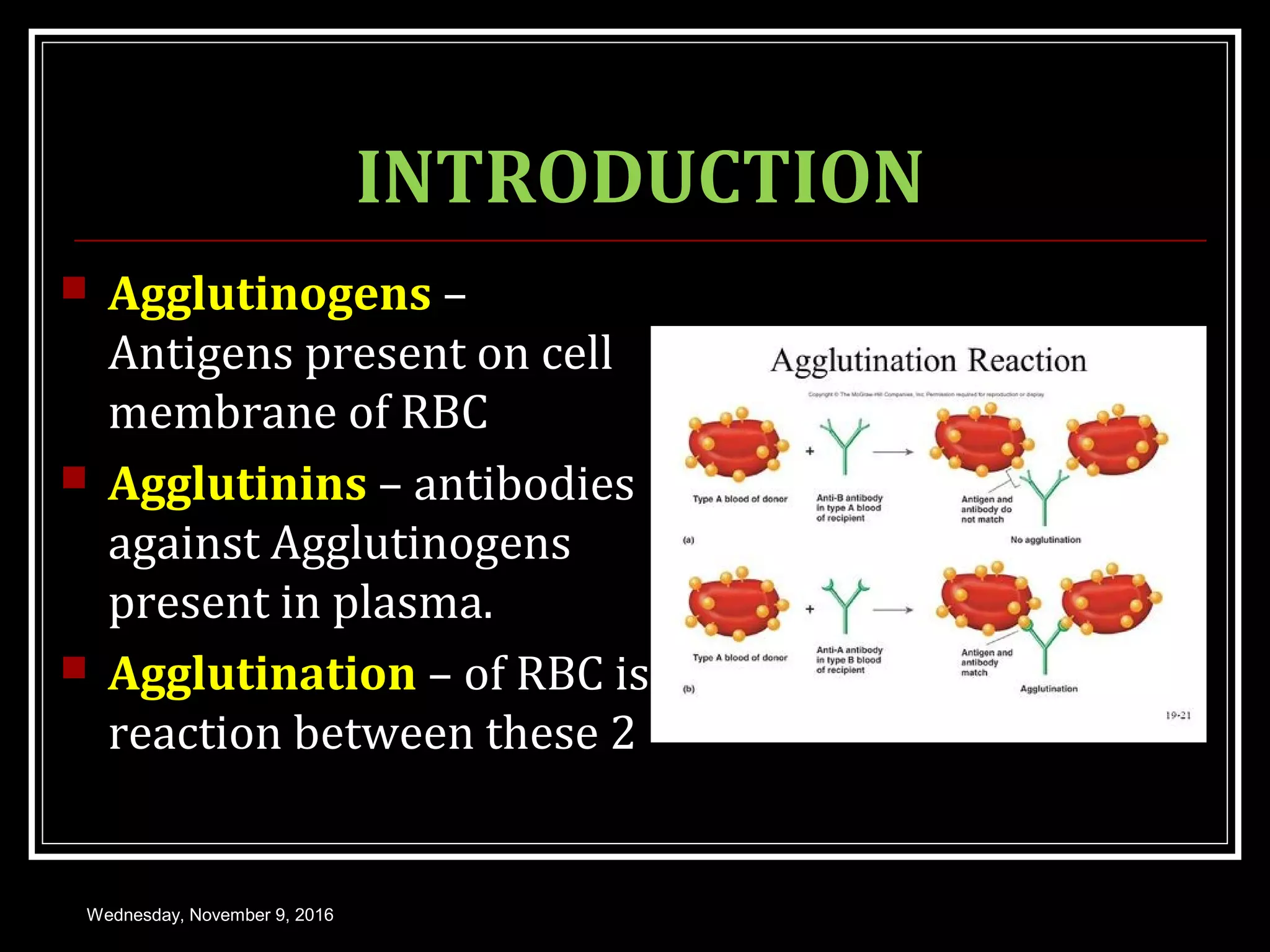


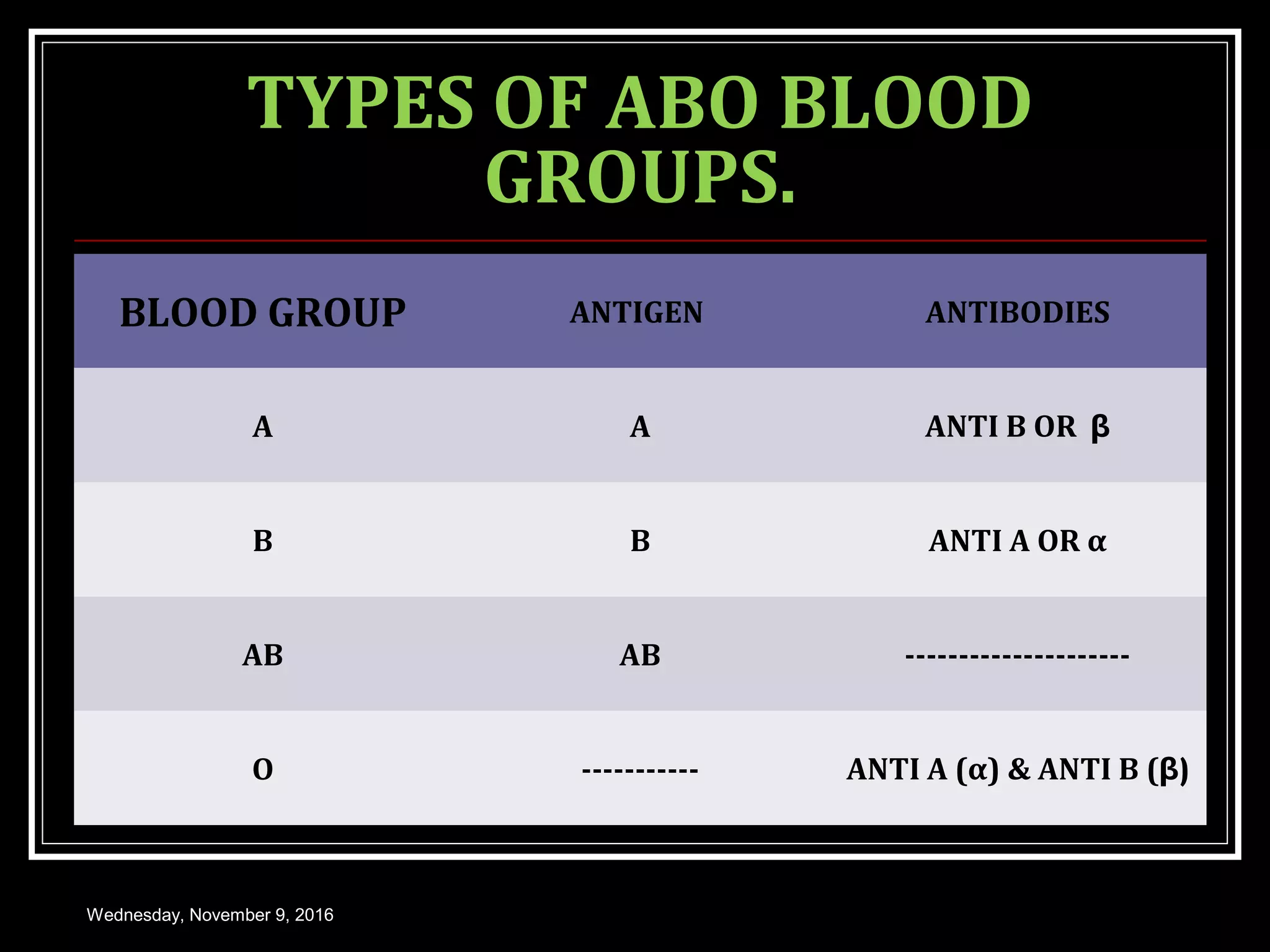
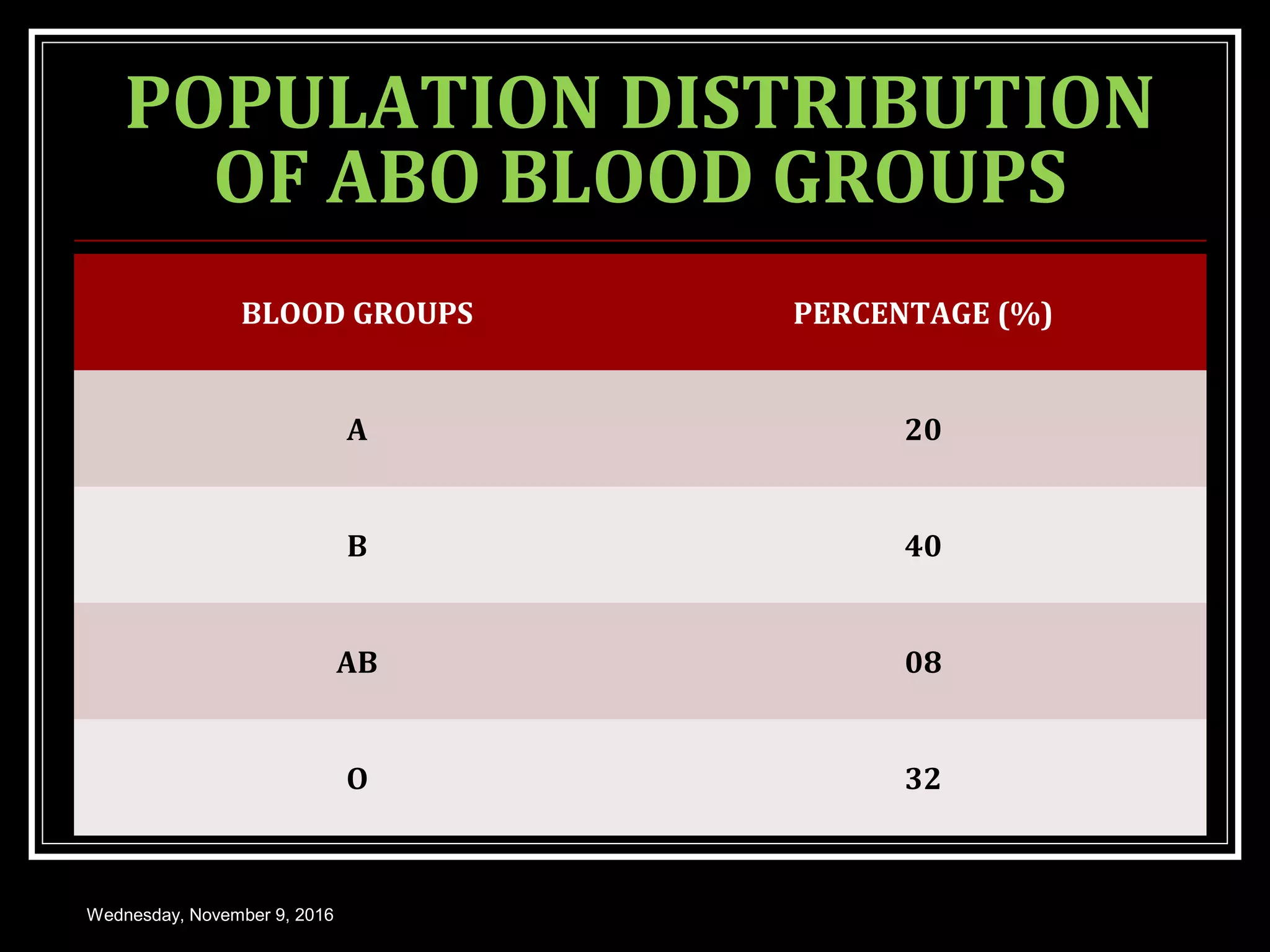
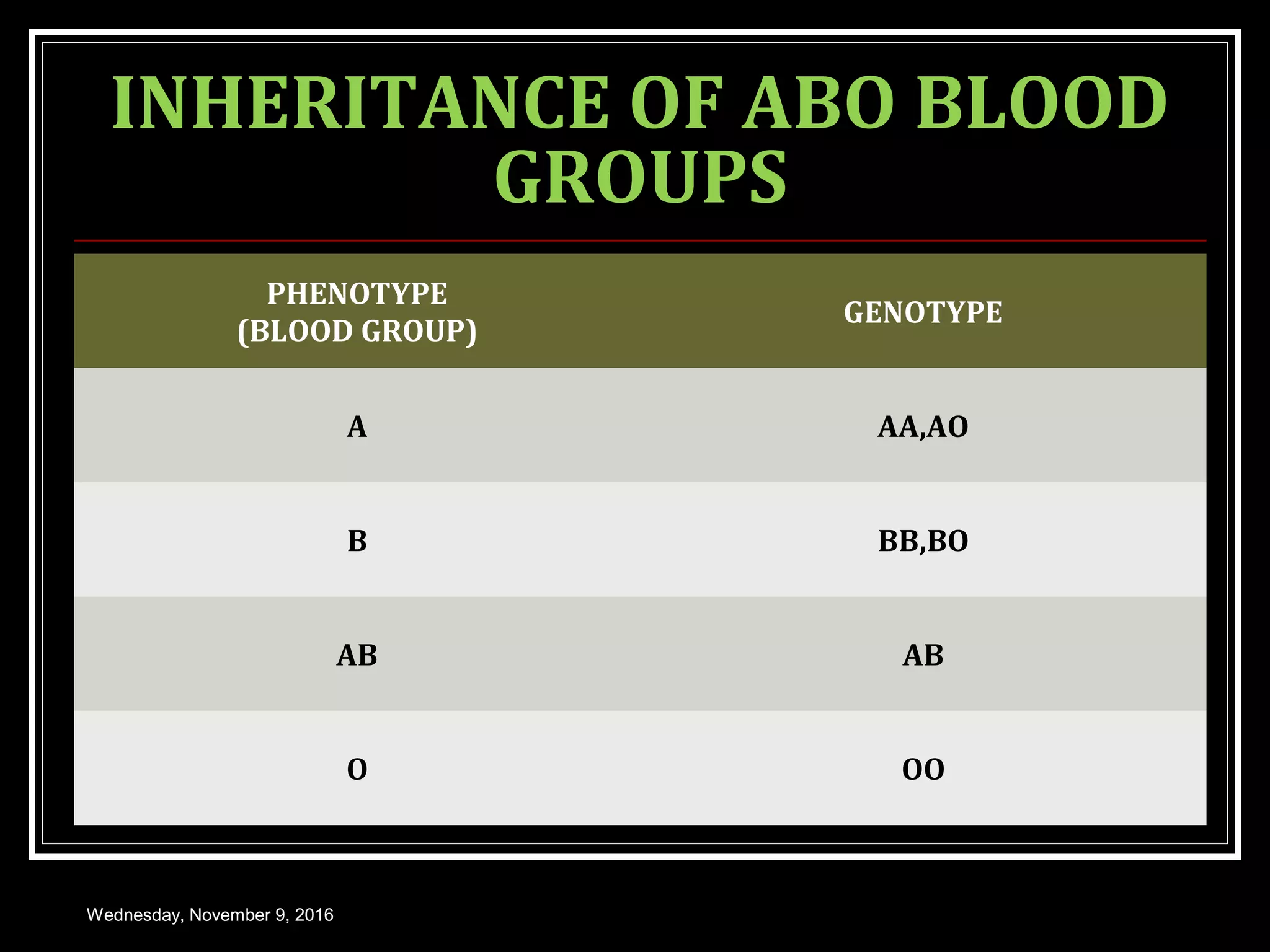


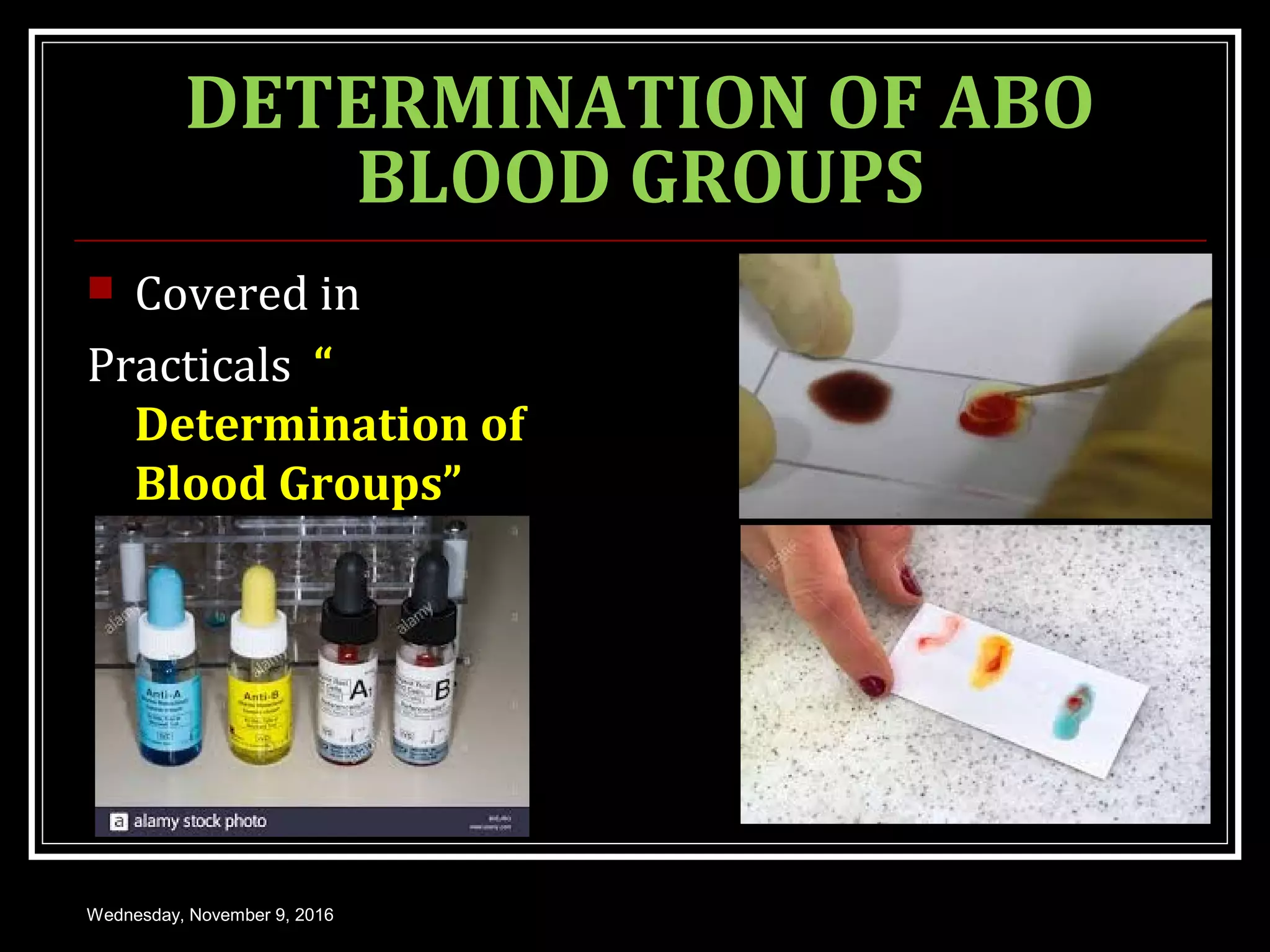
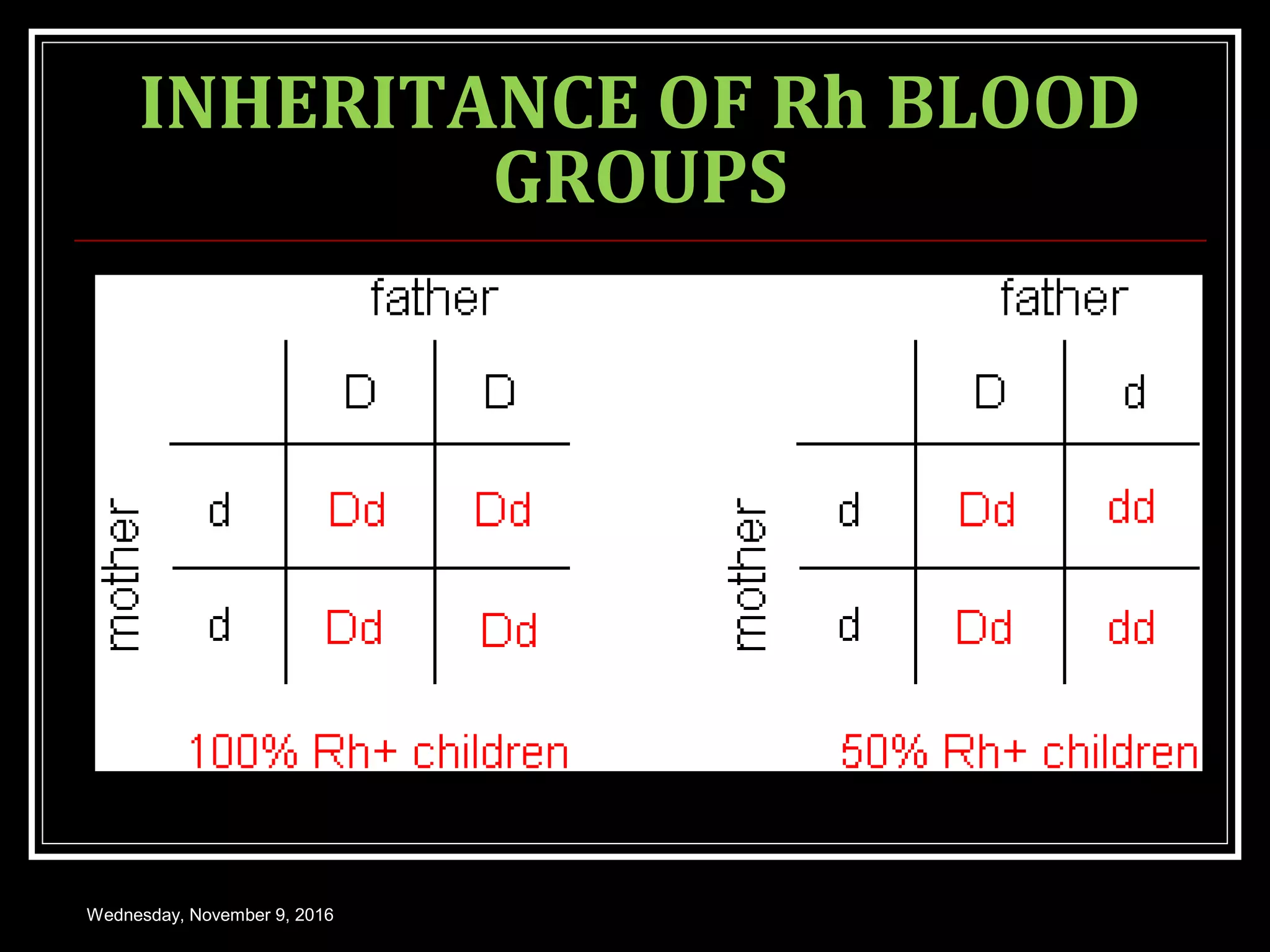










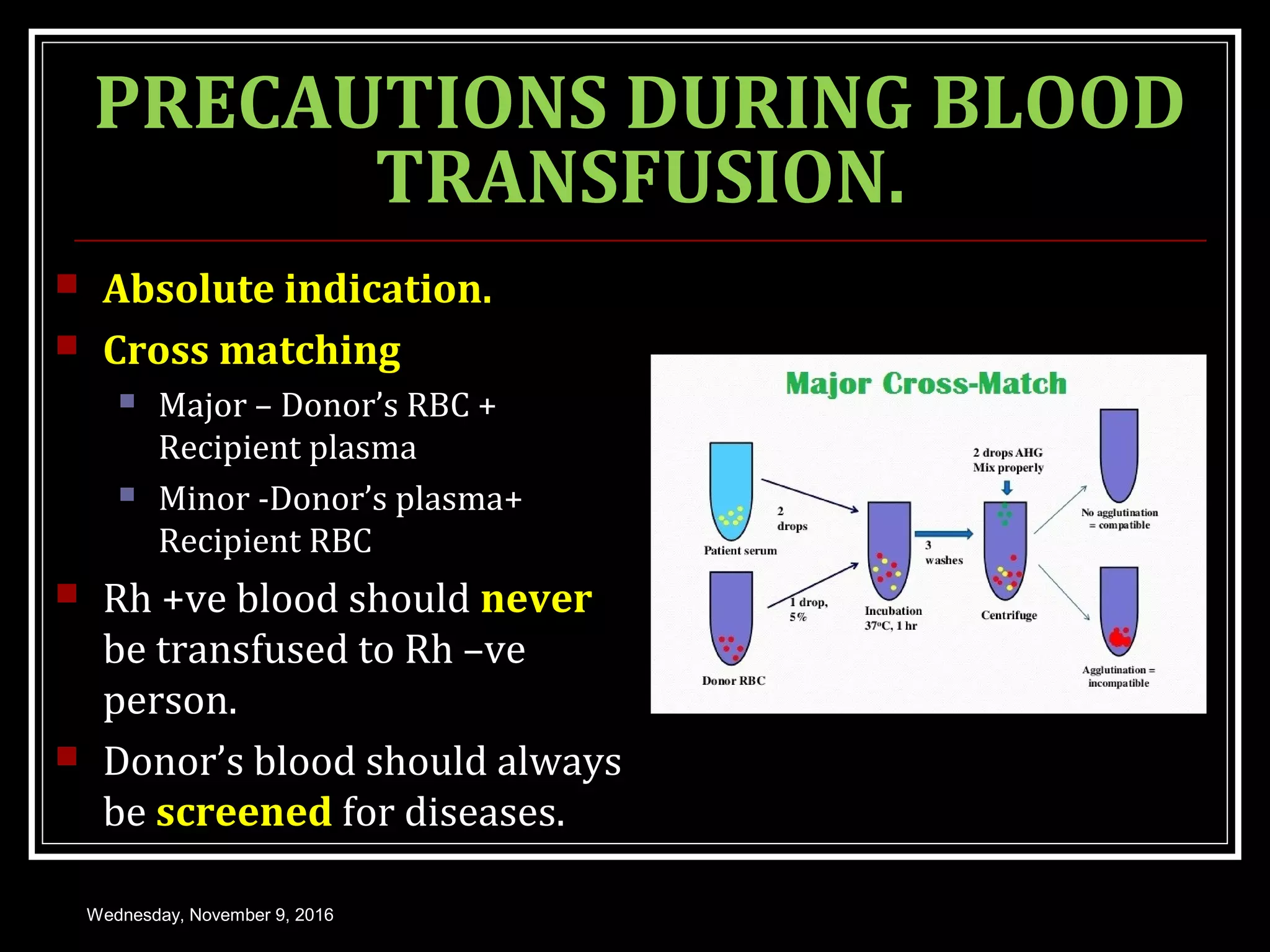






This document discusses blood groups and blood transfusions. It begins with an introduction to blood groups, including the ABO and Rh blood grouping systems. It describes the antigens and antibodies involved, inheritance patterns, and population distributions. It covers hemolytic disease of the newborn due to Rh incompatibility. The document also discusses blood transfusions in detail, including indications, donor and recipient selection, hazards, and storage of blood. It provides an overview of blood groups and transfusions with clinical and medical applications.