Downloaded 38 times
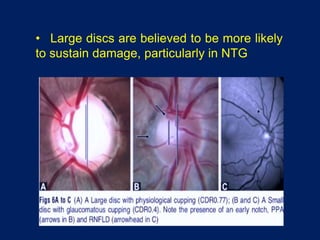
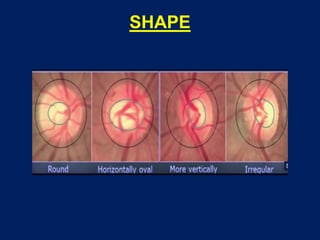
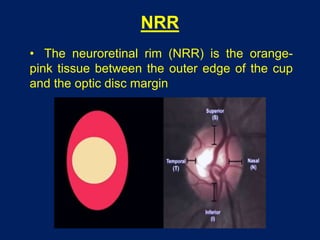
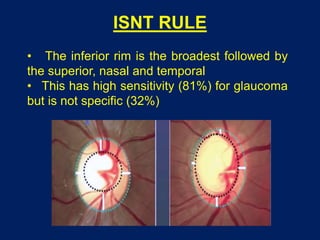
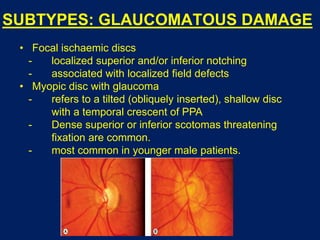
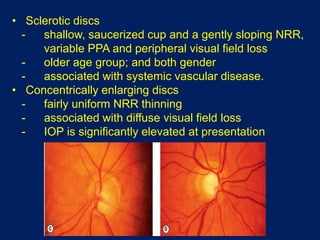
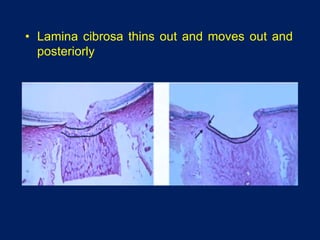

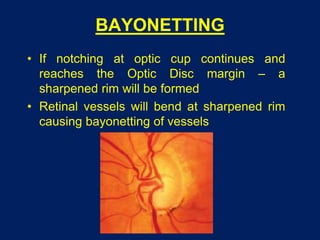
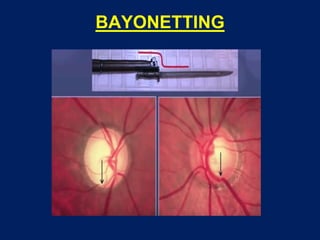
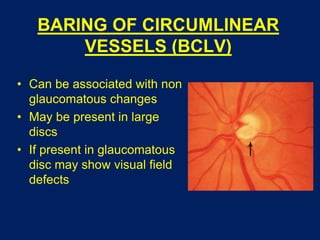
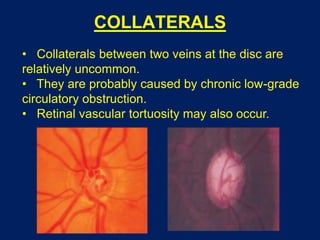
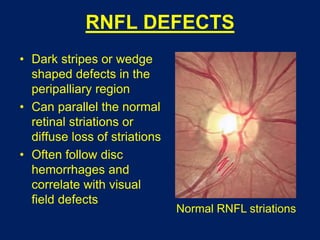
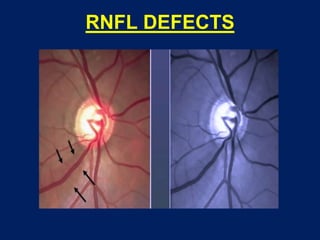
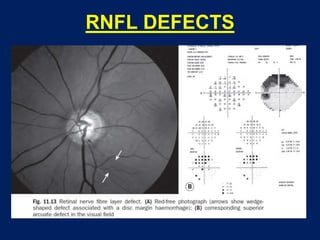
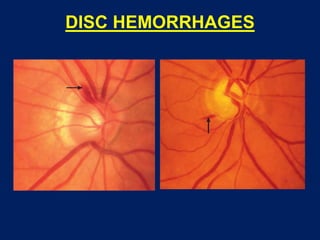

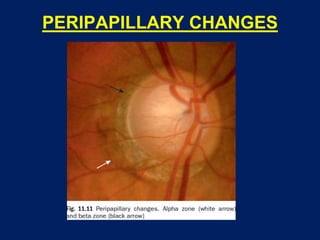
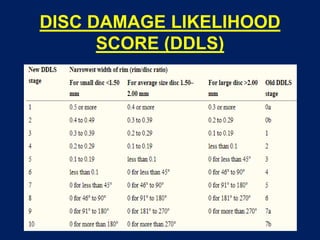
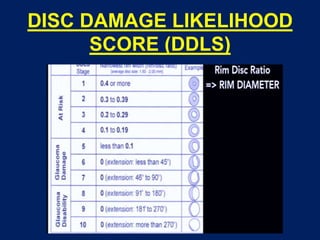


The document provides an overview of clinical evaluation of optic disc changes. It discusses examining the papillary changes including size, shape, neuroretinal rim, cupping and color. It also discusses vascular changes like nasalization of vessels and bayoneting of vessels. Peripapillary changes like RNFL defects, hemorrhages and gray crescent are also covered. The document outlines different staging systems to classify optic disc changes including the Disc Damage Likelihood Scale which quantifies glaucomatous damage based on rim width and disc size.