Downloaded 38 times
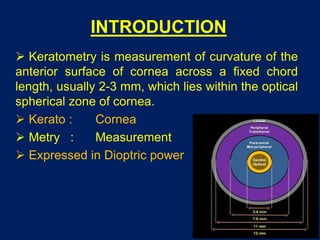
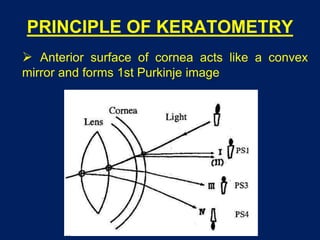









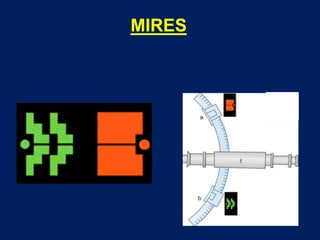
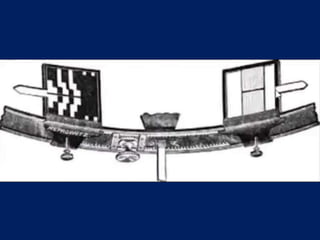

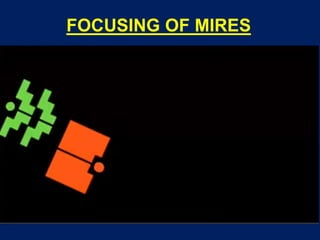

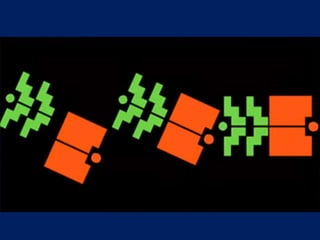

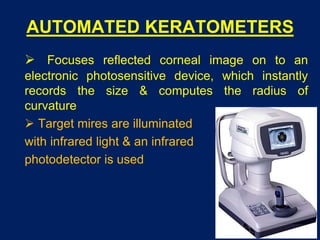



The document discusses keratometry, the measurement of the curvature of the anterior surface of the cornea, covering its principles, methods, and clinical applications. It describes both manual and automated keratometers, their advantages, and limitations, including common sources of errors in measurement. Key applications include assessing corneal astigmatism, guiding contact lens fitting, and monitoring corneal shape and post-surgical changes.






















































































