Downloaded 38 times
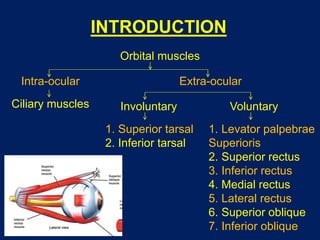

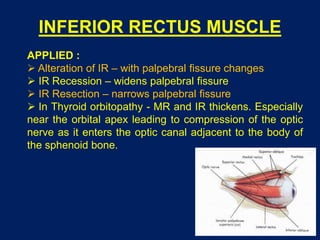
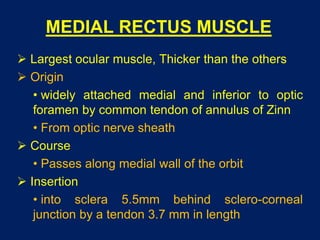
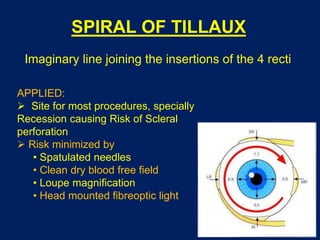
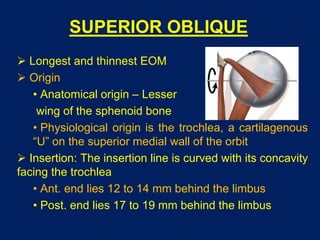
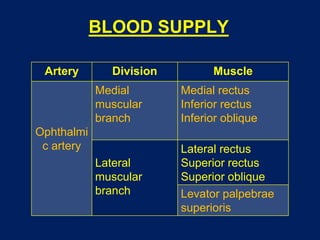
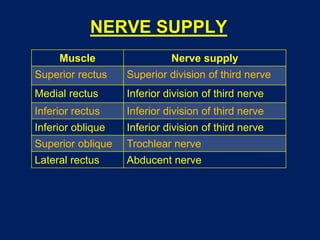
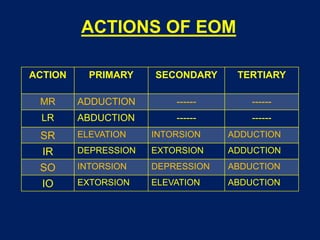
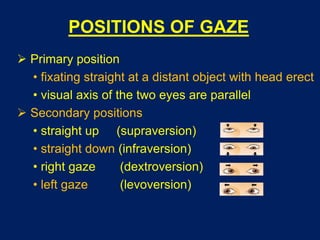

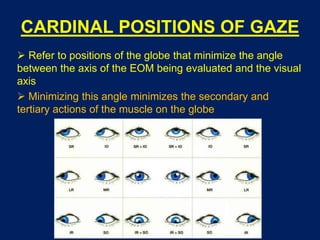
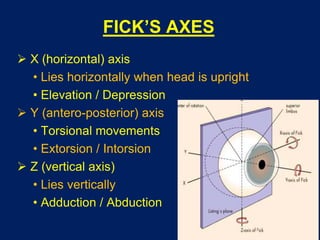
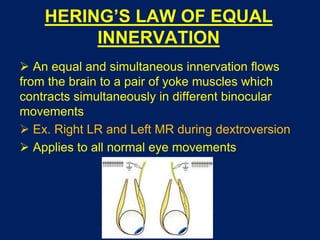
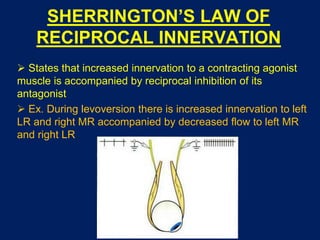


The document provides an overview of extraocular muscles (EOMs), including their embryology, anatomy, blood and nerve supply, actions, positions of gaze, and laws of ocular motility. It describes the seven EOMs - the four rectus muscles (superior, inferior, medial, lateral), two oblique muscles (superior, inferior), and levator palpebrae superioris. It discusses their origins, insertions, innervation and applied clinical concepts. Fick's axes, Listing's law, Donder's law, and Hering's and Sherrington's laws of innervation governing coordinated eye movements are also summarized.





















































































