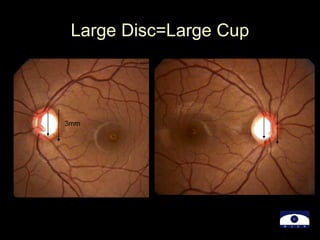
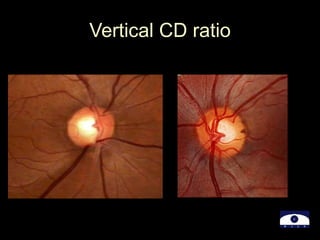
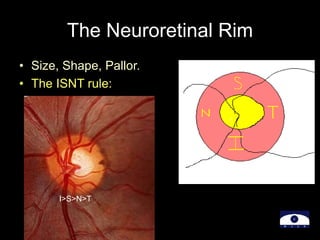
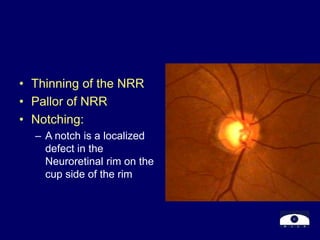
The document discusses the evaluation of the optic disc by Dr. Nirupama in the context of glaucoma diagnosis and management. It outlines the goals and methods of optic disc evaluation, key parameters to assess, and specific indicators of optic nerve damage such as neuroretinal rim changes and retinal nerve fiber layer defects. It emphasizes the importance of these evaluations in distinguishing between healthy and glaucomatous conditions and monitoring disease progression.