Presbyopia/ Methods of Presbyopic Addition Determination (healthkura.com)Bikash Sapkota
DIRECT DOWNLOAD LINK ❤❤https://healthkura.com/presbyopia-near-addition/❤❤
Dear viewers Check Out my other piece of works at ❤❤❤ https://healthkura.com ❤❤❤
Presbyopia and techniques of measurement
A fantastic presentation in the topic "Presbyopia and techniques of measurement"
A detailed information about presbyopia, techniques of presbyopic add determination and different correction methods.
Informative slide presentation on presbyopia for ophthalmology residents, ophthalmologists, optometrists, ophthalmic assistants, ophthalmic technicians, ophthalmic nurses, medical students, medical professors, teaching guides.
Presentation Contents:
--Introduction to presbyopia
-Types of presbyopia
-Risk factors
-Symptoms and signs
-Refractive error and presbyopia
-Methods of determining near add.
-Management of presbyopia
In a nutshell..
- The evaluation and management of presbyopia are important because significant functional deficits can occur when the condition is left untreated
- Undercorrected or uncorrected presbyopia can cause significant visual disability and have a negative impact on the pt.'s quality of life
- Finally, every tentative addition should be adjusted according to the particular needs of the patient
For Further Reading:
-Clinical Procedures in Optometry by J.D. Bartlett, J.B. Eskridge, J.F. Amos
-Primary Care Optometry by Theodere Grosvenor
-Borish’s Clinical Refraction by W.J. Benjamin
-Clinical Procedures for Ocular examination by Carlson et al
-American Academy of Ophthalmology
-Optometric Clinical Practice Guideline by American Optometric Association
-Internet
Follow me to get in touch with optometric and ophthalmic updates.
Accommodation/ Accommodation of Eye, Measurement of Accommodation of Eye (hea...Bikash Sapkota
CLICK HERE TO DOWNLOAD FULL PPT ❤❤ https://healthkura.com/measurement-of-accommodation-of-eye/ ❤❤
Dear viewers Check Out my other piece of works at ❤❤❤ https://healthkura.com ❤❤❤
Measurement of Accommodation of eye:
Amplitude, Facility,
Relative Accommodation, Fatigue, Lag,
Dynamic Retinoscopy
Presentation Layout:
-Introduction to accommodation of eye
-Mechanism
-Components
-Measurement of accommodation of eye
- Amplitude
- Facility
- Relative accommodation
- Lag
-Dynamic Retinoscopy
Accommodation
-dioptric adjustment of the crystalline lens of the eye
- to obtain clear vision for a given target of regard
-process by which the refractive power of eye is altered
- to ensure a clear retinal image
For further reading
-Clinical Procedures in Optometry by J.D. Bartlett, J.B. Eskridge, J.F. Amos
-Primary Care Optometry by Theodere Grosvenor
-Borish’s Clinical Refraction by W.J. Benjamin
-Clinical Procedures for Ocular examination by Carlson et al
-American Academy of Ophthalmology
-Optometric Clinical Practice Guideline by American Optometric Association
-Internet
Follow me to get in touch with optometric and ophthalmic updates
strabismus , gaze , ocular movements , classification etc
presented by senior optometrist & orthoptician at Sagarmatha Choudhary Eye Hospital, SCEH, LAHAN (NEPAL )
He explain details about the binocular gaze , EOMs, etc & work up of a patient of squint etc.
Presbyopia/ Methods of Presbyopic Addition Determination (healthkura.com)Bikash Sapkota
DIRECT DOWNLOAD LINK ❤❤https://healthkura.com/presbyopia-near-addition/❤❤
Dear viewers Check Out my other piece of works at ❤❤❤ https://healthkura.com ❤❤❤
Presbyopia and techniques of measurement
A fantastic presentation in the topic "Presbyopia and techniques of measurement"
A detailed information about presbyopia, techniques of presbyopic add determination and different correction methods.
Informative slide presentation on presbyopia for ophthalmology residents, ophthalmologists, optometrists, ophthalmic assistants, ophthalmic technicians, ophthalmic nurses, medical students, medical professors, teaching guides.
Presentation Contents:
--Introduction to presbyopia
-Types of presbyopia
-Risk factors
-Symptoms and signs
-Refractive error and presbyopia
-Methods of determining near add.
-Management of presbyopia
In a nutshell..
- The evaluation and management of presbyopia are important because significant functional deficits can occur when the condition is left untreated
- Undercorrected or uncorrected presbyopia can cause significant visual disability and have a negative impact on the pt.'s quality of life
- Finally, every tentative addition should be adjusted according to the particular needs of the patient
For Further Reading:
-Clinical Procedures in Optometry by J.D. Bartlett, J.B. Eskridge, J.F. Amos
-Primary Care Optometry by Theodere Grosvenor
-Borish’s Clinical Refraction by W.J. Benjamin
-Clinical Procedures for Ocular examination by Carlson et al
-American Academy of Ophthalmology
-Optometric Clinical Practice Guideline by American Optometric Association
-Internet
Follow me to get in touch with optometric and ophthalmic updates.
Accommodation/ Accommodation of Eye, Measurement of Accommodation of Eye (hea...Bikash Sapkota
CLICK HERE TO DOWNLOAD FULL PPT ❤❤ https://healthkura.com/measurement-of-accommodation-of-eye/ ❤❤
Dear viewers Check Out my other piece of works at ❤❤❤ https://healthkura.com ❤❤❤
Measurement of Accommodation of eye:
Amplitude, Facility,
Relative Accommodation, Fatigue, Lag,
Dynamic Retinoscopy
Presentation Layout:
-Introduction to accommodation of eye
-Mechanism
-Components
-Measurement of accommodation of eye
- Amplitude
- Facility
- Relative accommodation
- Lag
-Dynamic Retinoscopy
Accommodation
-dioptric adjustment of the crystalline lens of the eye
- to obtain clear vision for a given target of regard
-process by which the refractive power of eye is altered
- to ensure a clear retinal image
For further reading
-Clinical Procedures in Optometry by J.D. Bartlett, J.B. Eskridge, J.F. Amos
-Primary Care Optometry by Theodere Grosvenor
-Borish’s Clinical Refraction by W.J. Benjamin
-Clinical Procedures for Ocular examination by Carlson et al
-American Academy of Ophthalmology
-Optometric Clinical Practice Guideline by American Optometric Association
-Internet
Follow me to get in touch with optometric and ophthalmic updates
strabismus , gaze , ocular movements , classification etc
presented by senior optometrist & orthoptician at Sagarmatha Choudhary Eye Hospital, SCEH, LAHAN (NEPAL )
He explain details about the binocular gaze , EOMs, etc & work up of a patient of squint etc.
Motor evaluation tests of squint are mandatory for diagnosis and taking a decision. You have not to miss the proper techniques, tips and tricks of these tests (part 1)
Gives a very brief review of how to evaluate a case of squint in day to day clinical practice. How to diagnose a basic abnormality of the movement of eye.
This presentation is a detailed description of how a patient should be examined in an oprthoptic clinic. it lists down all the investigations sequentially. the order of investigations mentioned is the best way to investigate a squint case.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Ve...kevinkariuki227
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
TEST BANK for Operations Management, 14th Edition by William J. Stevenson, Verified Chapters 1 - 19, Complete Newest Version.pdf
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
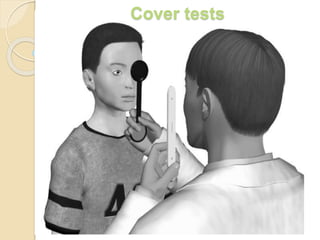
3. Foveal fixation in each eye, attention, cooperation, and the
ability to make eye movements are all necessary for cover
testing.
They allow the examiner to:
1) differentiate between tropia and phoria,
2) Asses the degree of control of deviation
3) Note fixation preference and strength of fixation of both eyes.
If a patient is unable to maintain constant fixation on an
accommodative target, cover tests should not be used.
3 types of cover tests:
1) cover-uncover test.
2) alternate cover test.
3) simultaneous prism and cover test.
4. It is typically performed by the ophthalmologist, orthoptist, or
ophthalmic technician.
The comprehensive cover test assessment is multifaceted.
Cover testing can be done to measure a deviation at near,
which requires an accommodative target held at a distance of
33cm for fixation.
It can also be done to measure a deviation with distance
fixation.
5. Detection of squint:
-a cover- uncover test is required to confirm a squint.
It has two components:
1) Observations to be made during covering. ( cover test )
2) Observations to be made during uncovering. ( cover-uncover
test )
7. Cover testing is the gold standard objective method for
determining the presence, type, and amount of ocular
misalignment (strabismus)
It is a monocular test.
It is simple to undertake, does not require great amounts of
skill by the examiner and is objective in nature
cover-uncover test is an objective determination of the
presence and amount of ocular deviation
Most important test for detecting manifest strabismus.
8. Also for differentiating a heterophoria from heterotropia.
Should be done for both distance and
near.
The single cover test is generally
performed first.
This is done by using an opaque or translucent (fogged)
occluder to occlude one eye.
9. In case of children it is the hand or a thumb which can be
used to avoid scaring them.
It is important to have a proper fixation target.
It should be a figure or letter of size 6/9 of snellen’s chart.
This is to control accommodation.
10. A fixation achieved by torch is not desirable.
The fixation distance should be 33cm for near and 6 meters for
distance.
As each eye is covered, the examiner watches for any
movement in the opposite, non-covered eye; such a movt
indicates a heterotropia. (cover test)
If there is no movt of the uncovered eye, movt of the covered
eye as the cover is applied and movt in opposite direction as
the cover is removed indicates a heterophoria. (Uncover test)
11. The uncover test is helpful in unmasking the latent squint
(heterophoria) which presents with both eyes appearing to
fixate the target.
One of the eyes is covered, which breaks the fusion, and if
there is any heterophoria the eye behind cover deviates.
(up/down/in/out)
The examiner then observes the behaviour of this eye as he
removes the cover.
If it remains deviated it confirms a latent squint with poor fusion
(poor recovery)
12. If it recovers the examiner observes for speed of recovery.
The speed of recovery indicates the strength of fusion and is
an important prognostic sign.
If the pt has a heterophoria, the eyes will be straight before
and after the cover-uncover test.
The deviation appears during the test.
13. This is because of interruption of binocular vision.
A pt with a heterotropia, however, starts with a deviated eye
and after testing end with the same eye or in case of alternate
heterotropia ,the opposite eye deviated.
In some pts with heterophoria, the eyes are straight before
testing, but they dissociate into a manifest deviation
(heterotropia) after the occlusion interrupts the binocular
vision.
14. Prerequisites for cover-uncover tests:
Ability of both eyes to fixate the target.
Ability of both eyes to have central fixation.
Ability of both eyes to have no gross / severe motility defect.
In presence of one eye being : blind/
markedley subnormal vision
/
severe restriction/
limitation movement /
an eccentric fixation,
which will not permit the eyes to refixate , the cover-uncover
test may be fallacious.
15. For infants, who would not allow an occluder or a
hand close to their face , the examiner can use
indirect occlusion test or distant cover test.
For children, very small pictures like those seen on a
Lang stick can be used.
Whereas for adults a small Snellen chart letter or
number can be used
Here the fixation target or light is obstructed for one
eye by an occluder at some distance away from the
16. Information from cover-uncover test:
Confirms a true manifest or latent squint and also its type: exo/
eso/ vertical deviation.
It also indicates the visual dominance or the presence of
amblyopia.
The examiner can detect even small angle squints leaving only
microtropia of < 5 prism dioptre deviation.
A cover- uncover test needs to be done in all nine cardinal
positions of gaze, as also for near and distance fixation
17. In a Manifest Strabismus it can tell us the following:
- The type of deviation: whether it be eso, exo, hyper, hypo or
cyclo tropia.
- The size of the deviation: slight, small, moderate or large
-Speed to take up fixation: if the eye takes up fixation fast it
means there is good vision in that eye
-Accommodation on the deviation
- Nystagmus
-Dissociated vertical deviation (DVD)
- Incomitance – deviation angle varies in each position of gaze.
18. In a Latent Deviation it can tell us the following:
esophoria,
exophoria,
-Type of deviation: hyperphoria,
hypophoria,
cyclophoria
- Size of deviation
- Rate of recovery that enables the person to achieve binocular
single vision.
- It also says about the strength of control over the deviation.
23. The alternate cover test is performed after the single cover test.
The alternate cover test is the most dissociative cover test and
measures a total deviation, including the tropic plus the
phoric/latent component.
This test is done to dissociate binocular fusion.
Alternately each eye is occluded and refixation movt of uncovered
eye to midline is observed.
No shift in alternate cover test indicates orthophoria.
A refixation shift to cover/alternate cover test indicates presence of
strabismus, either a tropia, phoria or a tropia with phoria.
Presence of a phoria is an indication of binocular fusion.
If no movement was seen on the unilateral cover test, but
movement is noted on the alternating test, the patient has a
phoria
27. The alternate prism cover test is similar to the alternate cover
test, with the addition of a prism held over one eye to quantify
the misalignment
Determines the amount of prism necessary to neutralize the
full deviation including any latent phoria, by quantitating the
shift associated with alternate cover testing.
A prism is placed in front of deviating eye with apex towards
the deviation.
Alternate cover testing is then done with prism in place.
The prism is changed ( either increased or decreased )
depending on the refixation shift.
28. Detects both latent and manifest deviations.
Testing should be performed at both distance and near
fixation.
Used to dissociate binocular fusion.
Deviation is quantified using prisms to eliminate the eye movt
as the occluder is switched from eye to eye.(prism alternate
cover test)
29. The misalignment is quantified with the size of the prism
(measured in Prism Diopters) which is required to neutralize
the deviation.
It may be necessary to use both horizontally and vertically
placed prisms.
This measures total deviation.
Does not distinguish between latent (heterophoria) and
manifest (hereotropia) components of deviation.
30. 2 horizontal or 2 vertical prisms should not be stacked
because doing so can induce significant measurment errors.
A more accurate method for measuring deviations larger than
those a single prism can correct is to place prisms in front of
each eye, although this is not perfectly additive either.
However, it is acceptable to stack a horizontal and vertical
prism over the same eye, if necessary.
If the pt head is tilted, the prisms must be tilted accordingly.
32. It is used to measure the tropia component of the monofixation
syndrome without dissociating the phoria.
Used in patients with small angle strabismus.
Performed by placing a prism in front of the deviating eye and
covering the fixating eye at the same time.
The test is repeated using increasing prism powers untill the
deviating eye no longer shifts.
The simultaneous prism and cover test provides the best
indication of the size of the deviation under real life conditions.
33. Common causes of variable measurements:
Poor control of accommodation.
Variable working distance
Tonic fusion not suspended.
Physiologic redress fixation movt.
Incomitant deviation.
34. Measurements should ideally be done in all 9 cardinal
position of gaze, especially for identifying and quantifying
incomitance.
Measuring the deviation in primary position, upgaze,
downgaze, right and left gaze, and with head tilt are sufficient.
Measurement of deviation in primary position should be done
at near (1/3 meter).
Plastic prisms are placed in the frontal position i.e, parallel to
infraorbital margin.
Glass prisms are placed in prentice position, i.e the posterior
surface of prism is perpendicular to the line of sight.
35.
36.
37. Cautions to be noted in avoidance of misdiagnoses
/contamination of results
It is important to avoid prolonged periods of dissociation of the
eyes until a diagnosis can be made regarding the strabismus.
Hence, the importance to note that although the eyes require
dissociation for a minimum of three seconds, that dissociation is
kept minimal whilst fixation is maintained.
In the case of intermittent or latent deviations, for dissociative
complications leading to misdiagnosis, it is also advised that
binocular vision is tested prior, along with stereo testing.
Frequently, during testing, the cover can be removed prematurely,
therefore as mentioned earlier; dissociation of at least three
seconds is needed for the patient to take up fixation during cover
testing.
This time allows for patients to recover from dissociation post
cover removal.
38. The use of a penlight should be utilized to observe the
steadiness and positioning of the deviated eye.
Ensure to assist the patient in maintaining fixation on
accommodative or distance targets at all times- if testing on
children or adults, request specific details pertaining to the
accommodative target (to assure accommodation is utilized) for
near testing.
Use of a detailed target for near fixation in both adults and
children will identify the effects of accommodation on the
deviation.
Observing pupillary constriction should also be indicative of
accommodation.
39. Cover-Uncover testing and alternate cover testing should be
performed on the deviating eye even when a constant
heterotropia is observed.
This practice ensures the detection of a consistent increase in
deviation and DVD isn’t neglected.
The presence of orthophoria in uncommon when assessing
both near and far fixation.
VA must be considered when there is no deviation seen upon
cover testing given amblyopic eyes may not take up fixation (VA
too poor to see target or eccentric fixation).
Microtropia may be present when a small unequal VA is
recorded.