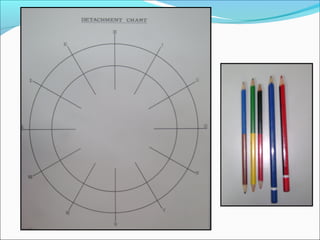
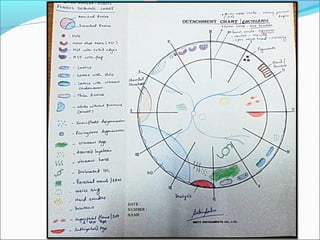
The document outlines techniques for retinal drawing used by retinal surgeons to document fundus pathology, emphasizing the importance of fundus evaluations including optic disc and retinal vasculature assessments. It details the methodology for creating retinal charts, showing various retinal conditions through the use of color-coded annotations. Additionally, it highlights steps for accurately depicting lesions in relation to the optic nerve and other landmarks.