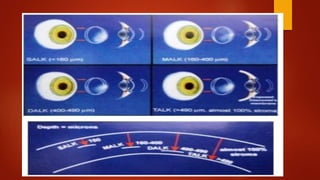
Lamellar keratoplasty involves replacing only a partial thickness of the diseased cornea, sparing the healthy posterior layers. It is less invasive than penetrating keratoplasty. Anterior lamellar keratoplasty techniques aim to replace the anterior corneal layers above Descemet's membrane for conditions like scars, dystrophies, or infections. The big bubble technique using injected air is effective at separating the layers, while viscoelastic dissection and hydrodelamination are alternatives. Outcomes depend on the dissection method and surgeon experience.