Downloaded 38 times

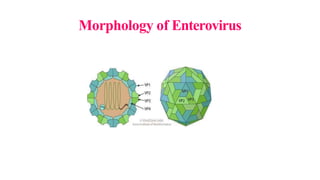
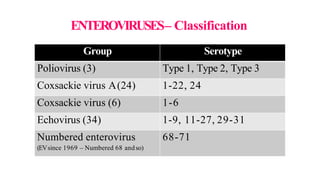
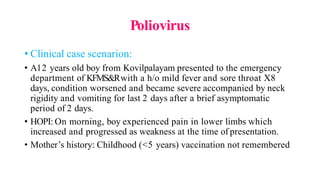
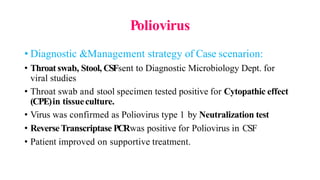
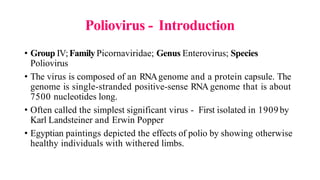





This document provides an overview of picornaviruses, with a focus on poliovirus. It begins by outlining the objectives of discussing picornavirus morphology, classification, pathogenesis, and the clinical manifestations, diagnosis, treatment and prevention of poliomyelitis and other diseases caused by echoviruses and rhinoviruses. It then provides details on picornavirus morphology, classification, the history of poliovirus research and discovery, epidemiology, characteristics, cultivation, pathogenesis, and clinical features of poliomyelitis. Key points covered include that poliovirus is an enterovirus that can cause paralysis, replication in the gastrointestinal tract and nervous system, and that infection may be asymptomatic, minor



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















