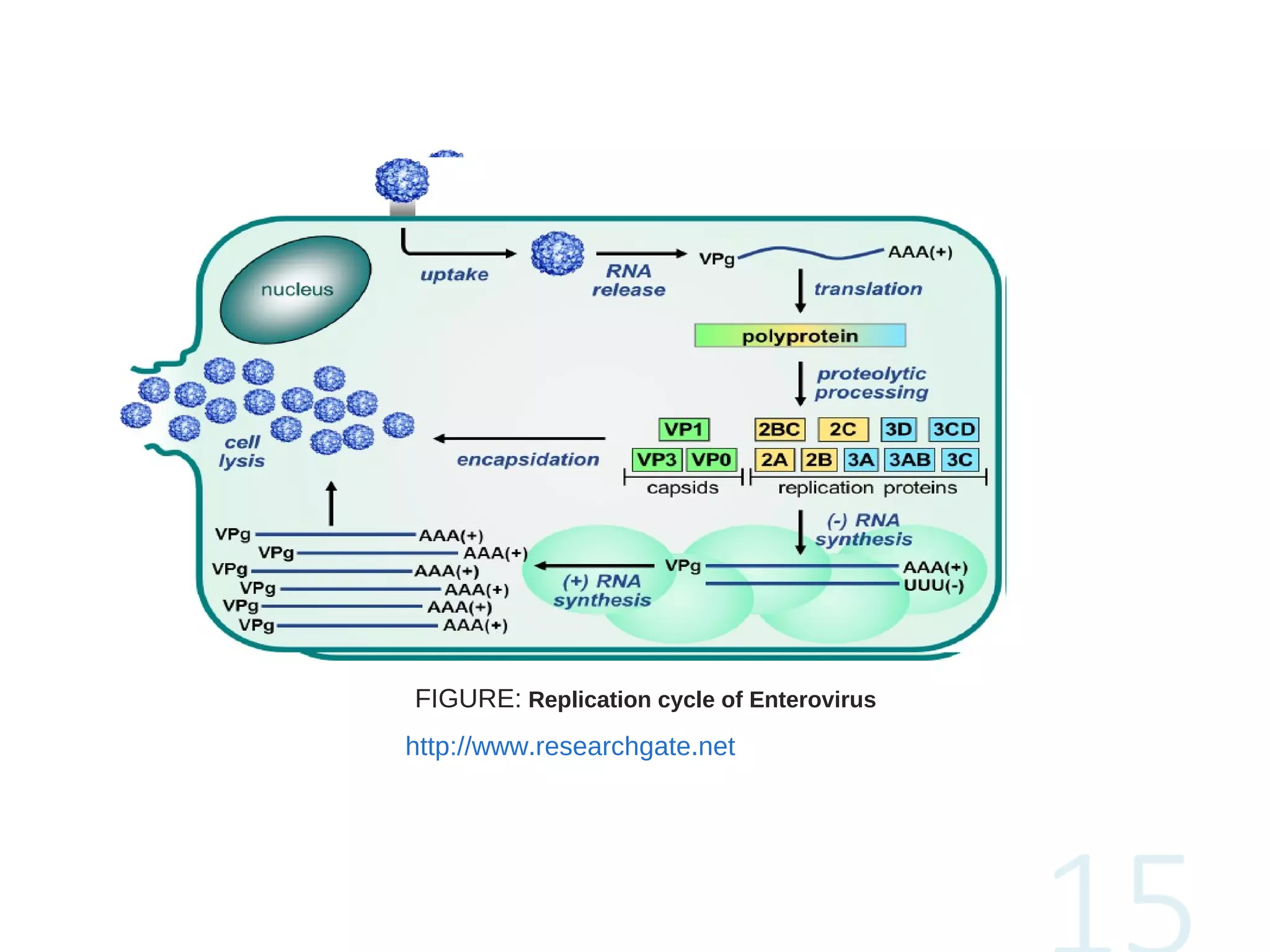
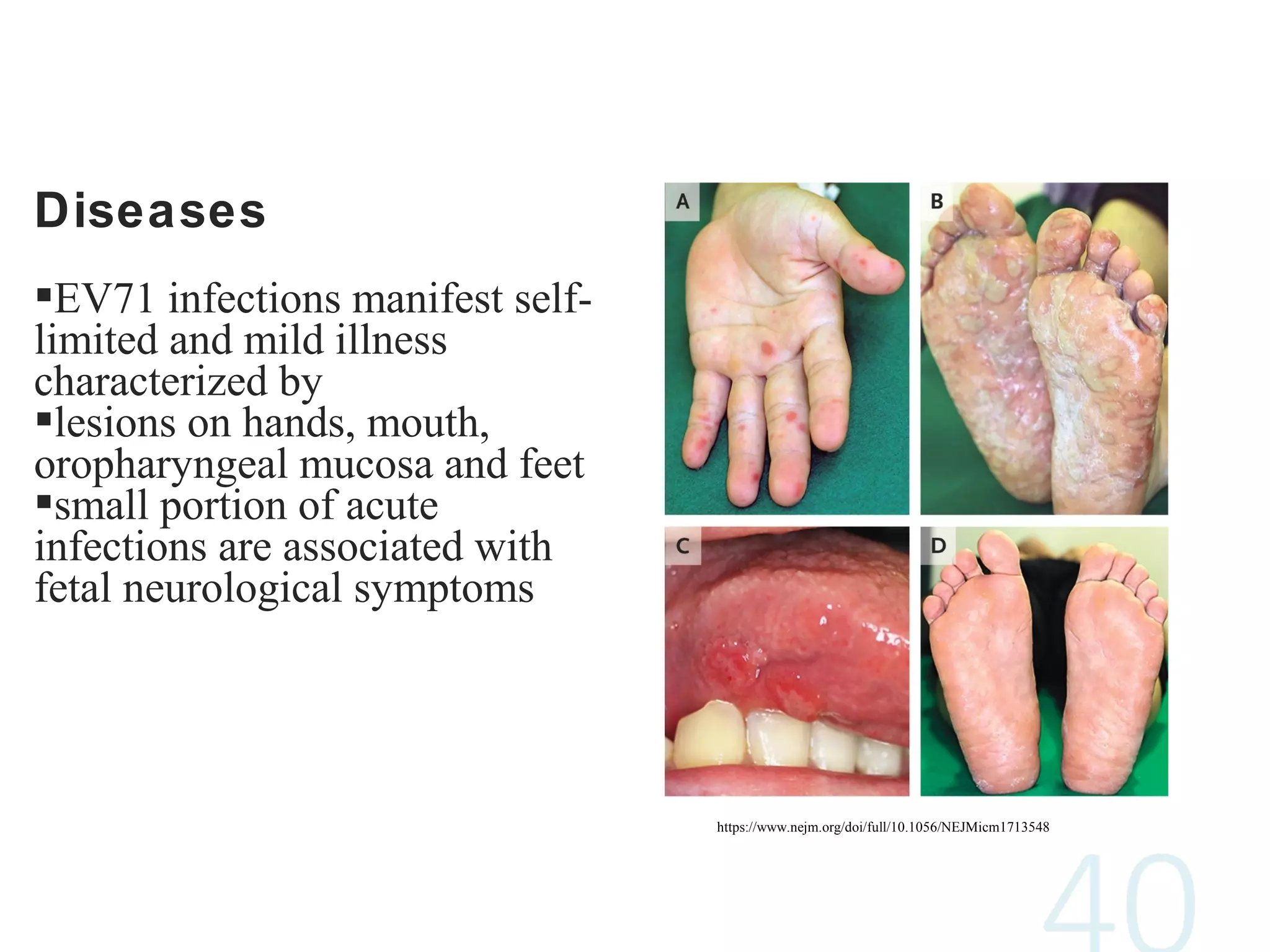
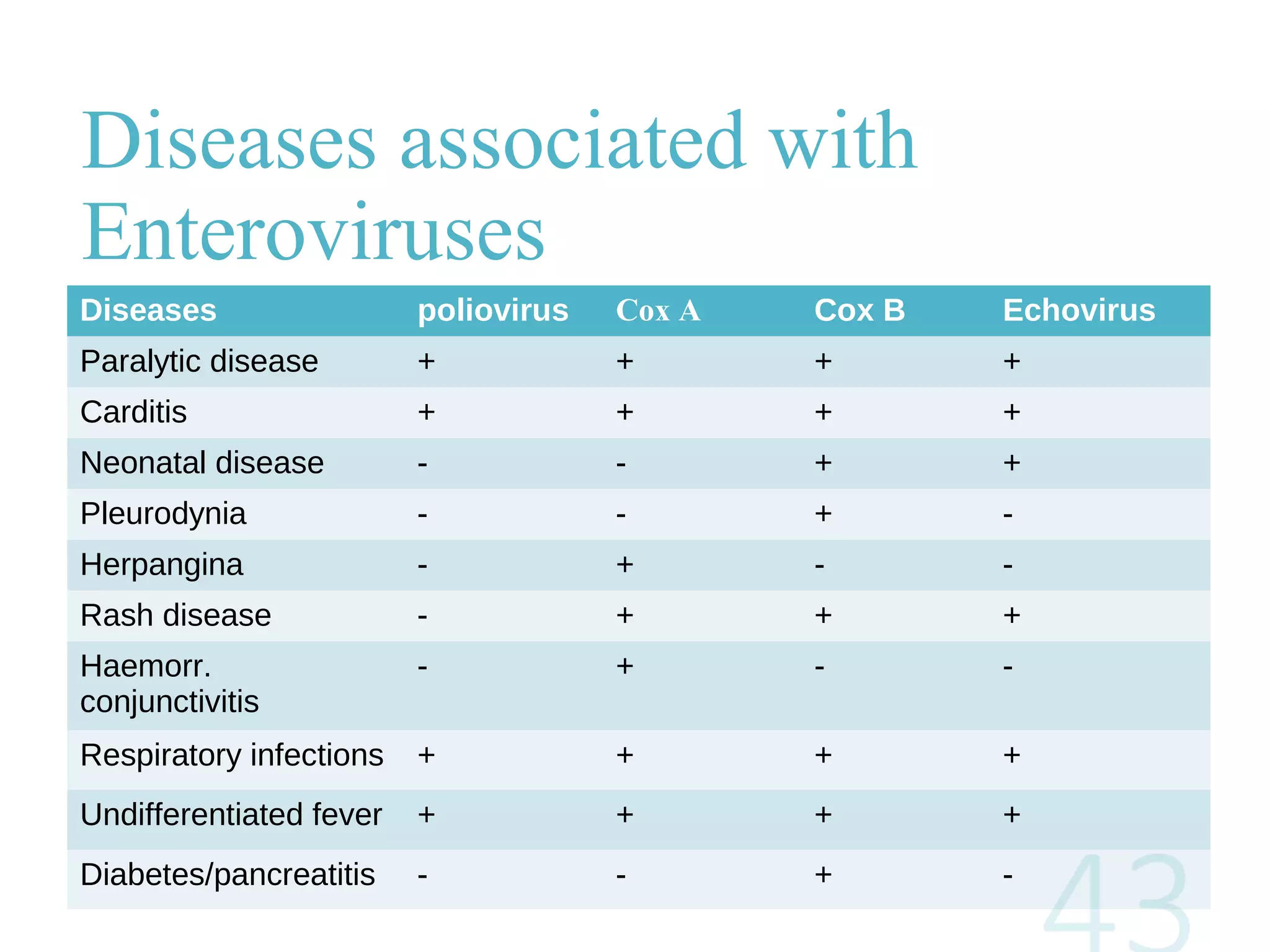
Enteroviruses are a genus of viruses that include poliovirus, coxsackieviruses, echoviruses, and newer human enteroviruses like EV-68. They are small, non-enveloped viruses that enter the host and replicate in the gastrointestinal tract or central nervous system, causing a variety of mild to severe diseases. Common illnesses include respiratory infections, rashes, meningitis, and myocarditis. While vaccination has eradicated polio in most countries, other enteroviruses continue to circulate globally and cause periodic outbreaks of diseases.