Downloaded 62 times

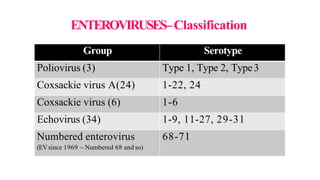
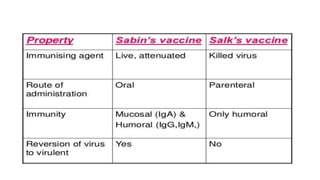
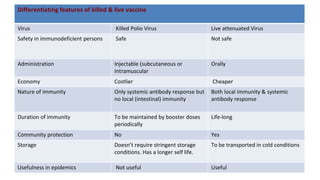
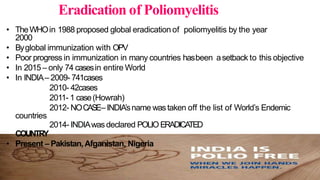
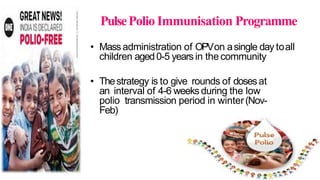





The document provides a comprehensive overview of the Picornaviridae family of viruses, focusing on poliovirus and its impact on human health. Poliomyelitis, caused by poliovirus types 1, 2, and 3, primarily spreads through the fecal-oral route and can result in serious neurological diseases, though most infections are subclinical. Vaccination strategies, including the Salk and Sabin vaccines, are essential for prevention, and global efforts have significantly reduced the incidence of polio, especially in countries like India.























































































