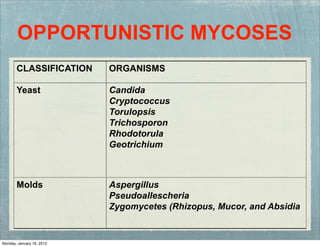

1. The document discusses various opportunistic mycoses including Candida, Aspergillus, and Zygomycetes. 2. It provides classifications of the organisms, compares true pathogenic fungi to opportunistic fungi, and describes various clinical manifestations including oral and disseminated candidiasis, allergic and systemic aspergillosis, and mucormycosis. 3. Laboratory diagnosis, culture characteristics, and treatment options are covered for each type of mycosis.



































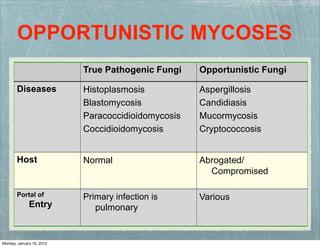
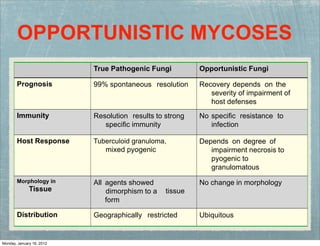
![Opportunistic_mycoses.pptx[1]qwersfdfsgbrfg.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/opportunisticmycoses-251113162005-6d43351d-thumbnail.jpg?width=640&height=640&fit=bounds)