Downloaded 369 times





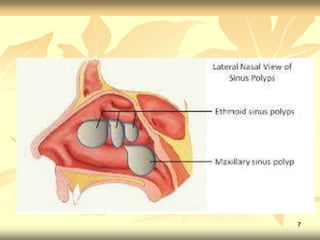











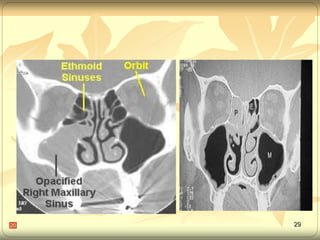



Nasal polyps are abnormal lesions that originate from the nasal mucosa or paranasal sinuses. They are most commonly caused by chronic inflammation from various sources. Nasal polyps present with symptoms like nasal obstruction, postnasal drip, and headaches. Investigations include CT scans, nasal endoscopy, and tests for conditions like cystic fibrosis. Treatment options include oral steroids, sinus surgery to remove polyps, and addressing underlying causes of inflammation. While surgery provides relief, nasal polyps often recur due to the chronic inflammatory nature of the condition.











































































































