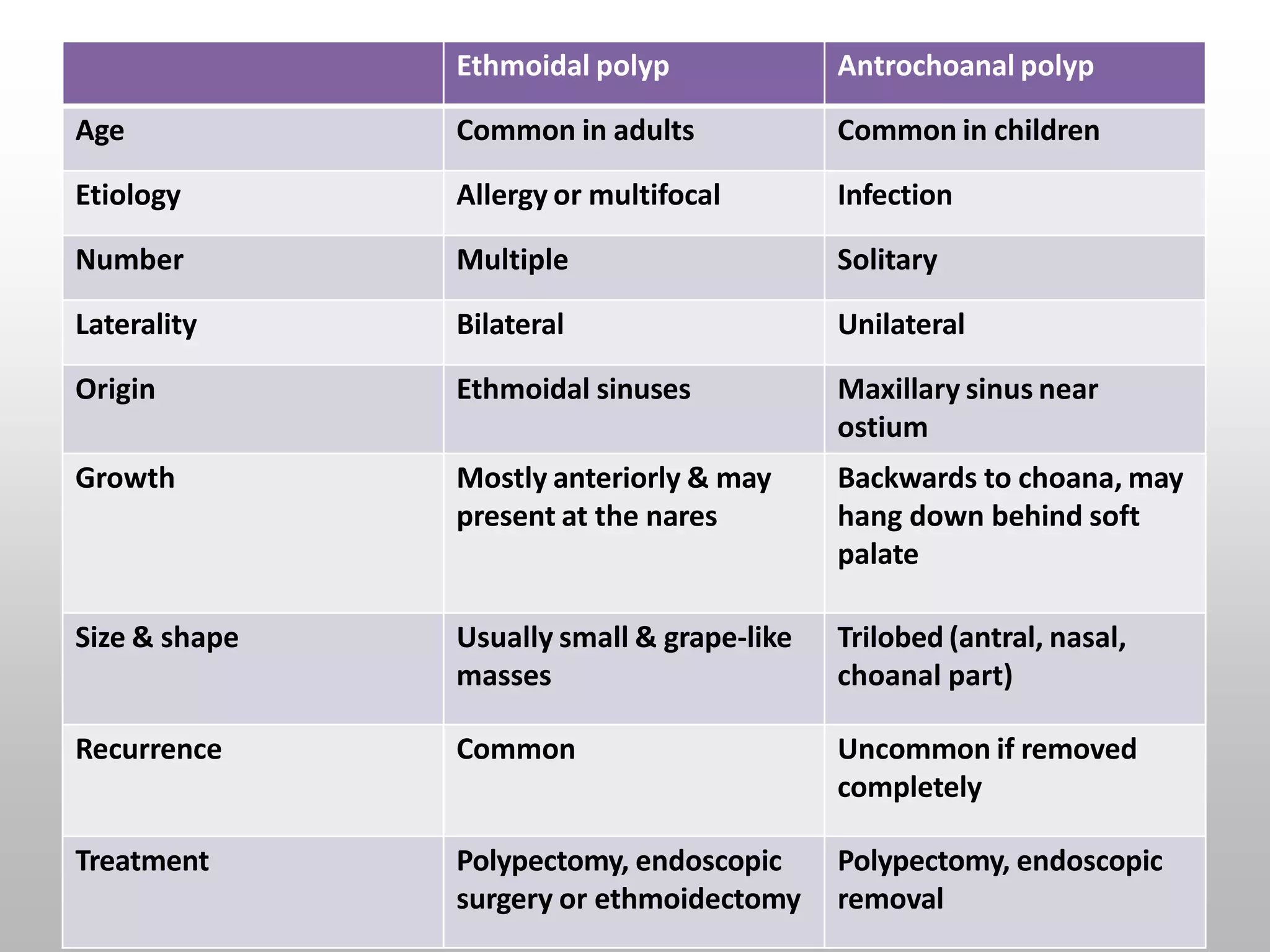
This document discusses nasal polyps and antrochoanal polyps. It defines nasal polyps as non-neoplastic masses of edematous nasal or sinus tissue. The main types are bilateral ethmoidal polyp and antrochoanal polyp. Nasal polyps are commonly caused by inflammatory conditions like rhinosinusitis or disorders of ciliary motility. Antrochoanal polyps originate in the maxillary sinus near its ostium. Symptoms include nasal obstruction, loss of smell, and discharge. Treatment involves polypectomy, intranasal ethmoidectomy, or endoscopic sinus surgery depending on the type and location of polyp.