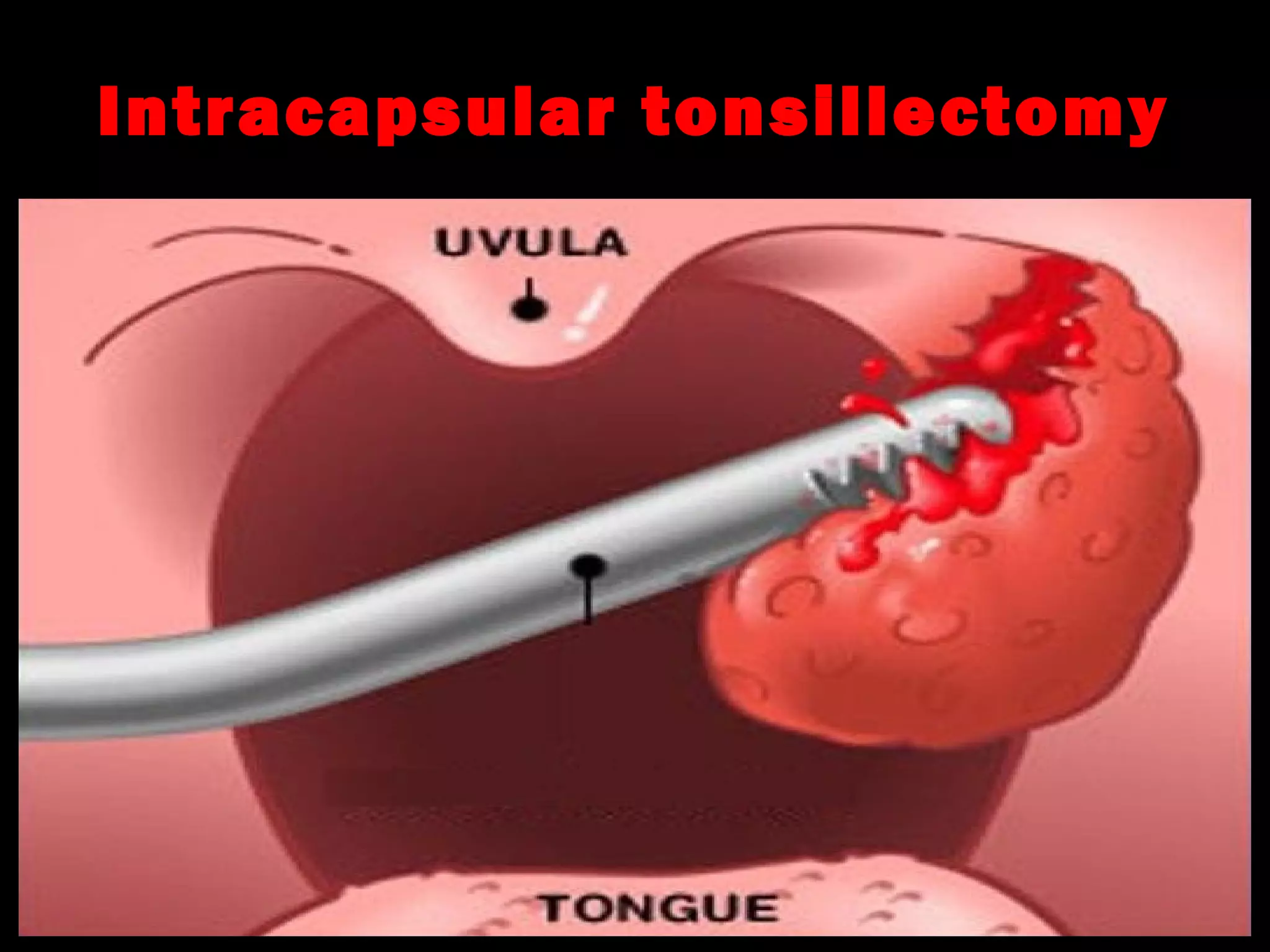
1) Tonsillectomy and adenoidectomy are common ENT procedures used to treat recurrent tonsillitis, sleep apnea, and other conditions. The history of these procedures dates back to ancient times, but modern techniques use electrocautery, lasers, or other methods.
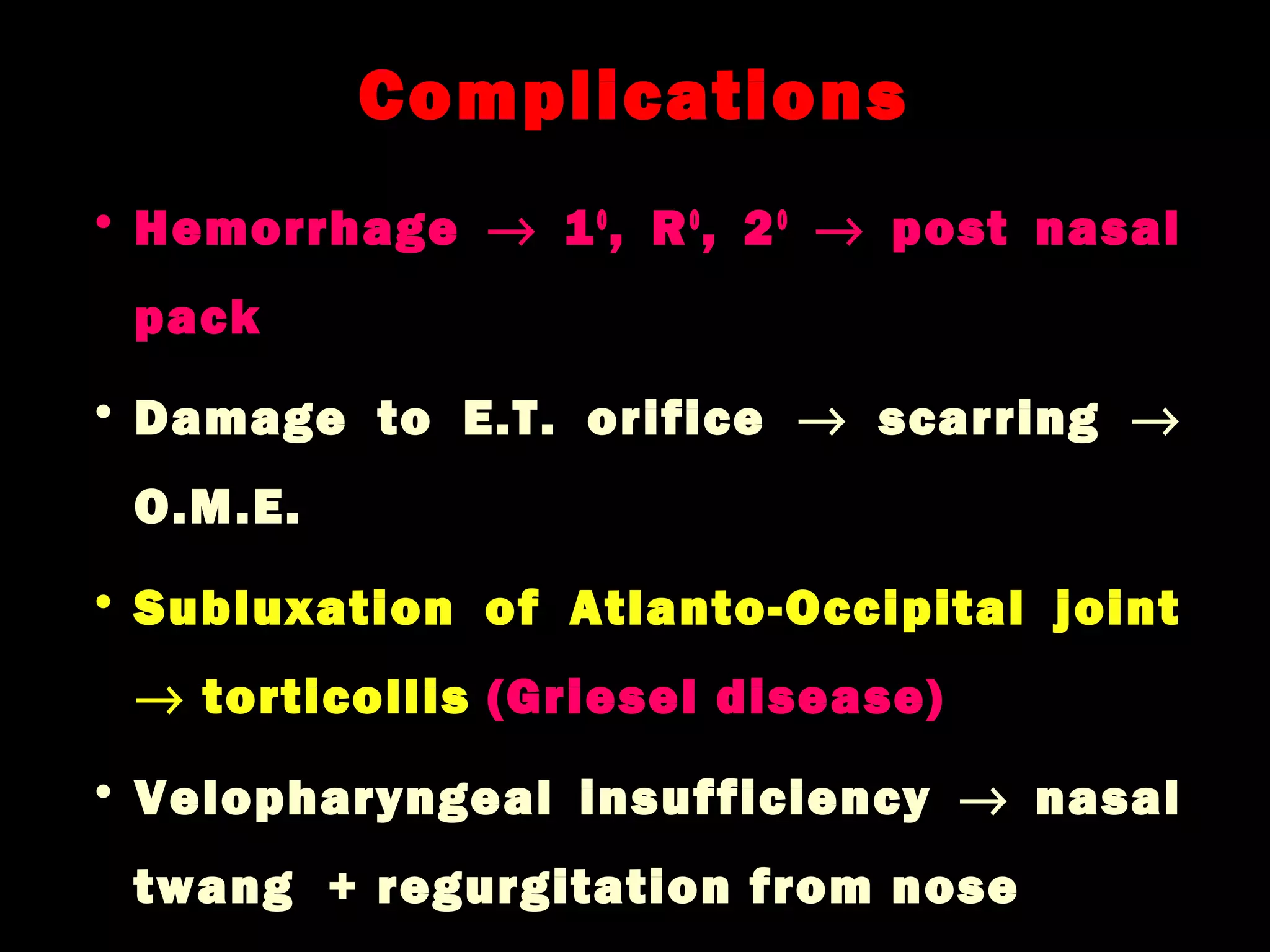
2) Complications can include bleeding, infection, and in rare cases injury to nearby structures like the uvula. Proper postoperative care and monitoring for bleeding is important.
3) A peritonsillar abscess (quinsy) occurs when a tonsillar infection spreads, causing a pocket of pus. Treatment involves antibiotics, needle drainage if large enough, or incision and drainage surgery. Recurrent or