Download to read offline
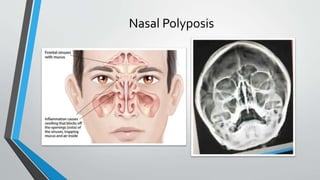





The document discusses nasal polyposis, an inflammatory condition characterized by the formation of nasal polyps, which are soft, jelly-like overgrowths of mucosa. It outlines the types, etiology, incidence, clinical features, pathogenesis, and treatment options for nasal polyps, emphasizing the importance of endoscopic surgery and medical treatment post-surgery. Additionally, it highlights the antrochoanal polyp, its characteristics, symptoms, and recommended surgical intervention.































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)














