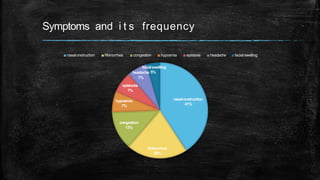
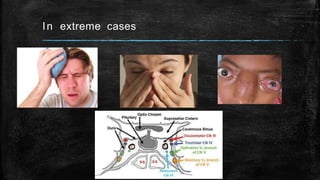
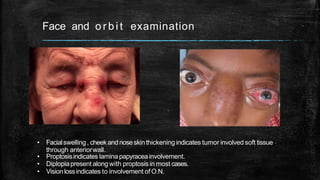
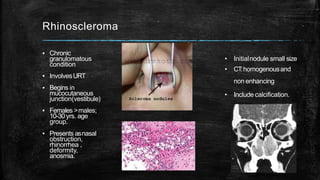
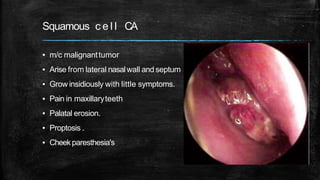
1. Nasal masses can present with symptoms like nasal obstruction, rhinorrhea, congestion, hyposmia, and epistaxis. Physical examination may reveal facial swelling, proptosis, or diplopia depending on site and extent of the mass.
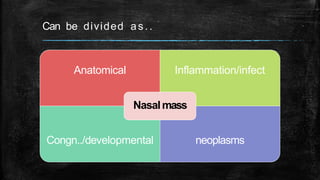
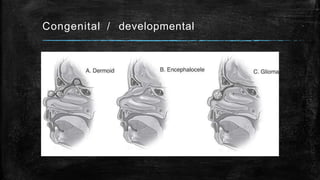
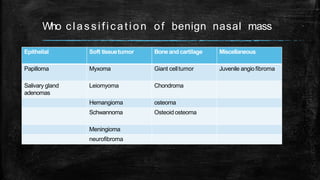
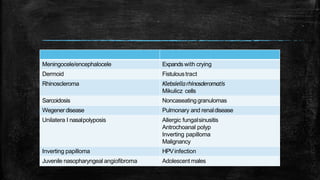
2. Nasal masses can be anatomical variants, inflammatory/infectious, congenital/developmental, or neoplasms. Common nasal masses include nasal polyps, inverted papilloma, juvenile angiofibroma, and lymphocytic hypophysitis.
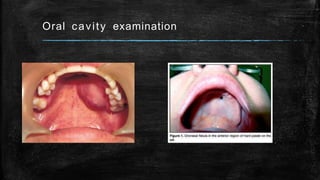
3. Diagnostic evaluation includes nasal endoscopy, CT scan, and biopsy. CT is helpful for surgical planning. Differential diagnosis depends on clinical features and may