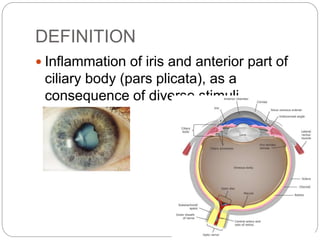
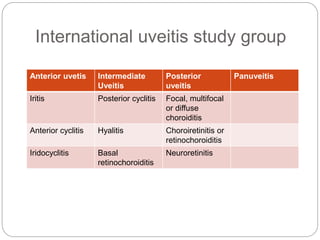
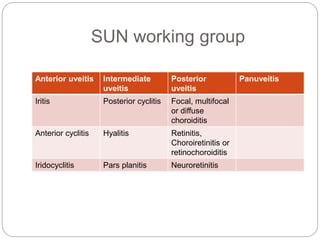
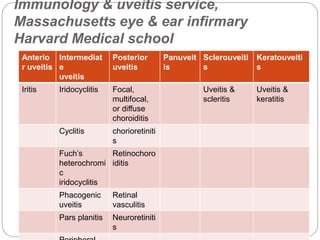
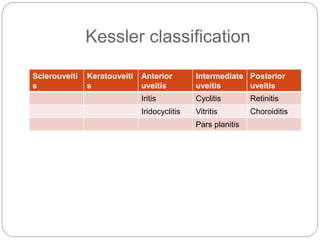
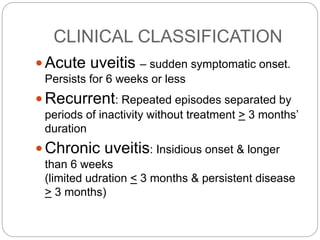



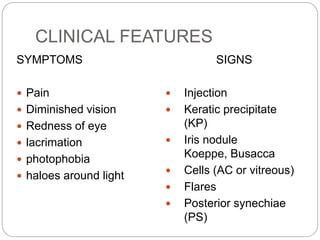



Dr. TP Chhangte discusses anterior uveitis, including its definition, epidemiology, classification, pathology, clinical features, complications, and differential diagnosis. Some key points: - Anterior uveitis is inflammation of the iris and anterior part of the ciliary body. Its prevalence has been increasing and it commonly affects people aged 20-50. - Uveitis can be classified anatomically, clinically, etiologically, and pathologically. The anatomical classification divides uveitis into anterior, intermediate, posterior, and panuveitis based on location of inflammation. - Clinical features of anterior uveitis include eye pain, redness, photophobia, and decreased vision. On examination






































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


