Downloaded 23 times


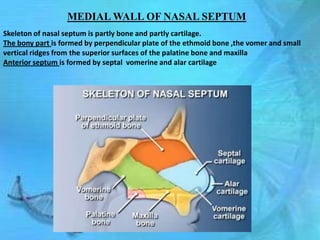
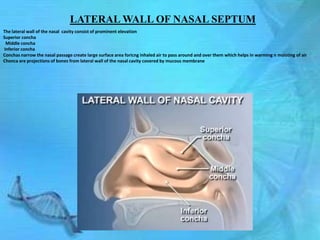
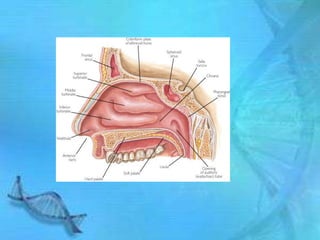
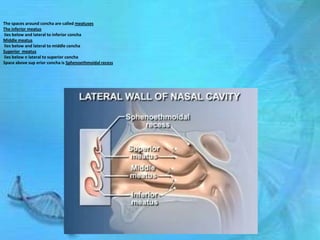
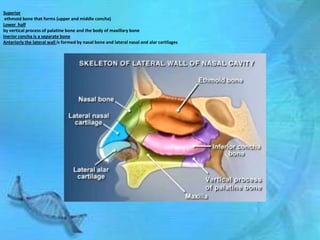
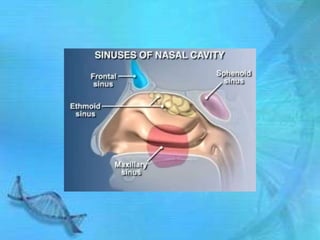
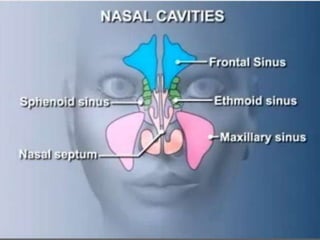
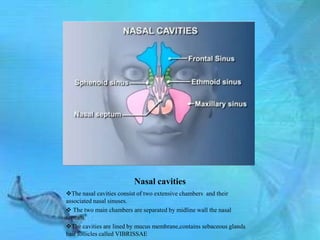

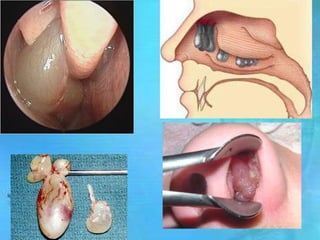
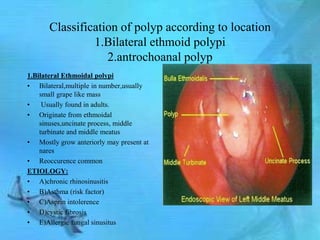
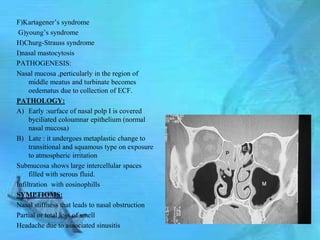
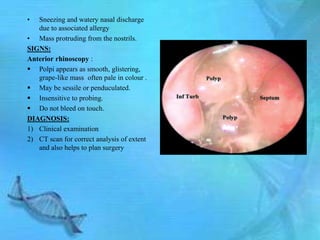


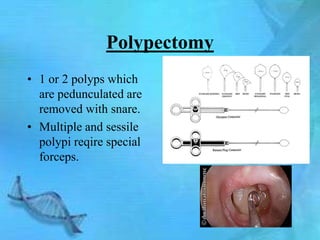

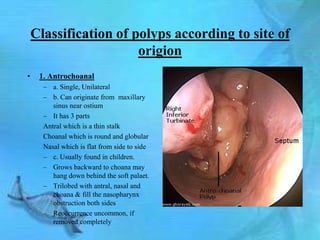
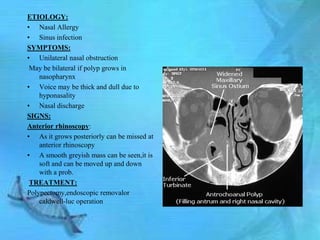
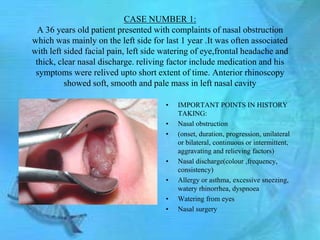
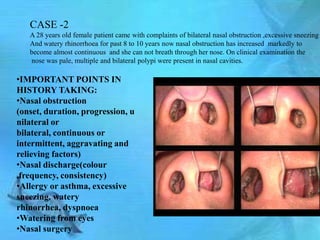
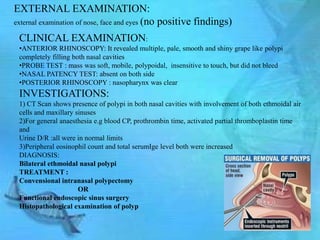
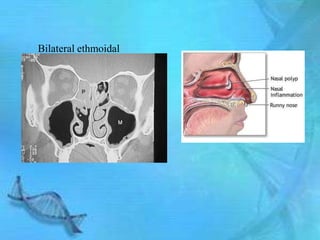


This document provides information about nasal polyps through three parts. Part 1 discusses the anatomy of the nasal cavity and its relationship to polyps. It describes the structures of the nasal septum and lateral walls. Part 2 defines nasal polyps and classifies them according to location. It also discusses their etiology, pathogenesis, symptoms, signs, diagnosis and treatment options. Part 3 presents two case studies of patients presenting with nasal polyps - one involving an antrochoanal polyp and the other involving bilateral ethmoid polyps. Both cases discuss the relevant history, examination findings, investigations, diagnoses and treatment plans.


































































