Downloaded 1,845 times





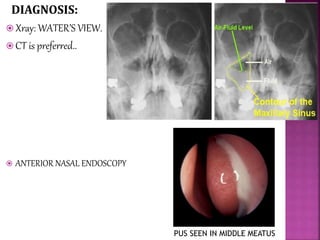







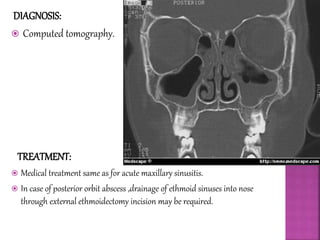

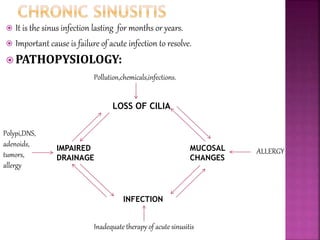

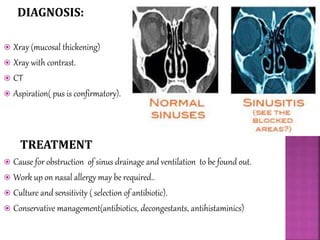

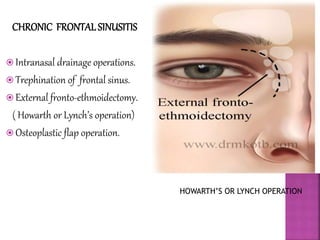


This document provides information on sinusitis, including: 1) It defines sinusitis as inflammation of the sinus mucosa and lists the most commonly involved sinuses. Bacterial causes are noted. 2) Predisposing factors for sinusitis include local obstructions that inhibit drainage as well as general factors like poor health and environment. 3) Diagnosis involves imaging like x-rays and CT scans. Treatment includes antibiotics, nasal decongestants, and surgery in some cases.