Downloaded 88 times
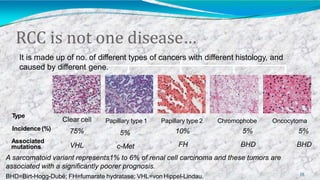


Renal cell carcinoma accounts for approximately 3% of adult solid malignancies in the US, with over 51,000 new cases and 12,900 deaths annually. It arises from renal tubular epithelium and includes several subtypes associated with different genetic mutations and prognoses. Surgery is the main treatment for localized disease, while advanced or metastatic renal cell carcinoma has a poor prognosis despite newer targeted therapies and immunotherapies that have improved outcomes.























































































