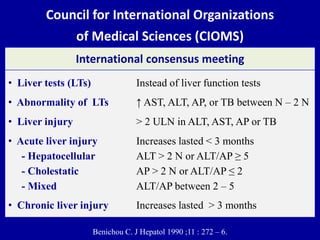
1) Liver tests are elevated in 10-50% of patients with inflammatory bowel disease (IBD). This can be due to the IBD itself, its treatment, or unrelated factors.
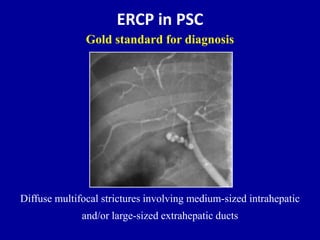
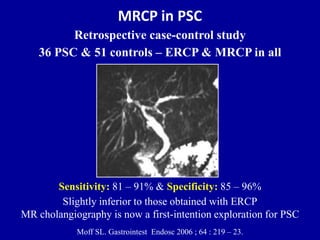
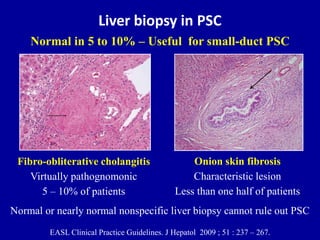
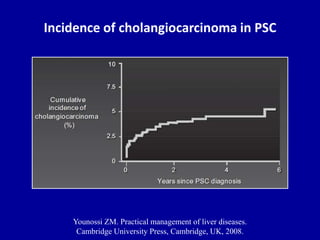
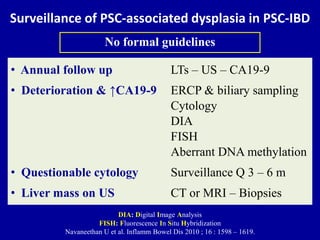
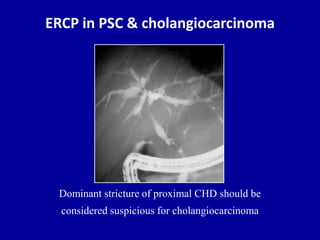
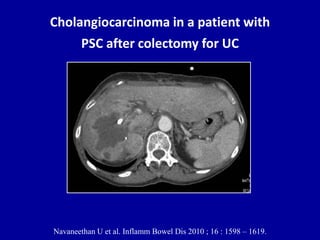
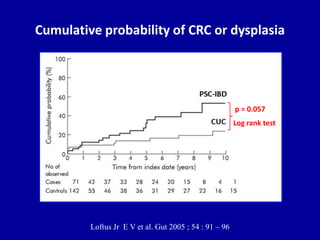
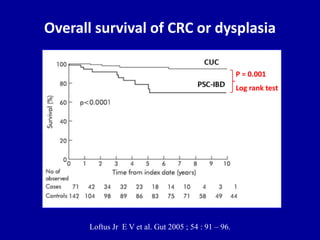
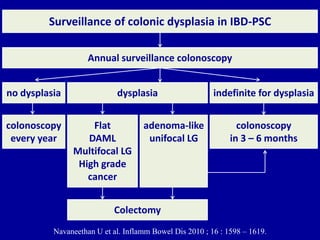
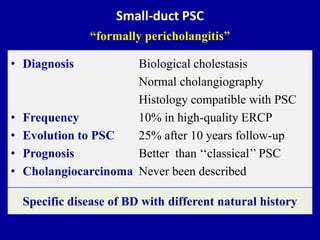
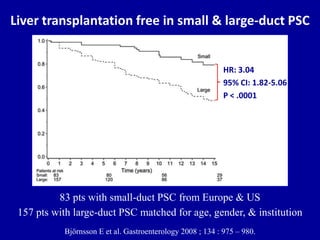
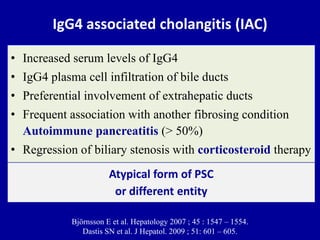
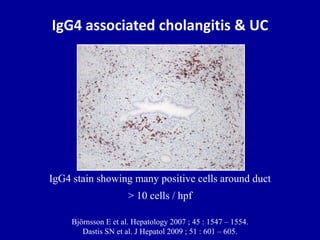
2) Primary sclerosing cholangitis (PSC) is a liver condition strongly associated with IBD. Screening and surveillance is important for PSC patients due to increased risk of cholangiocarcinoma.
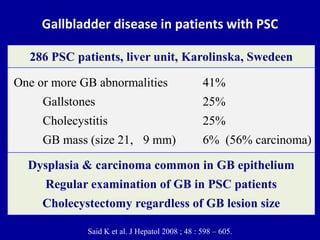
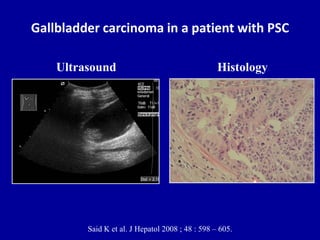
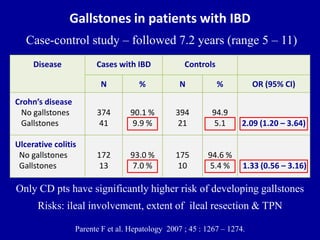
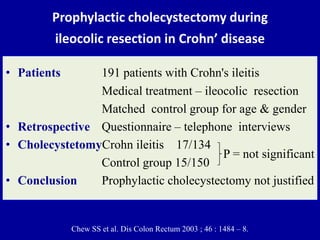
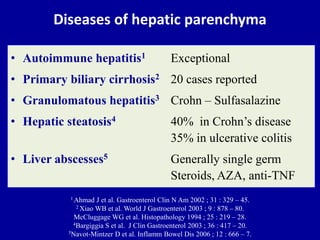
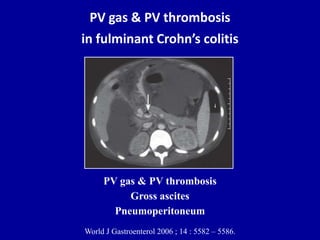
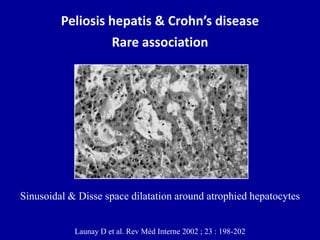
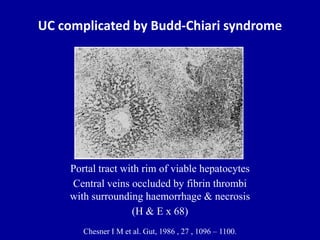
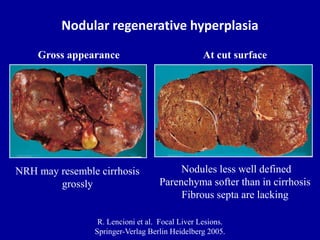
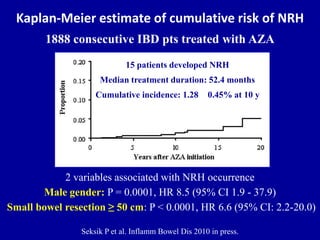
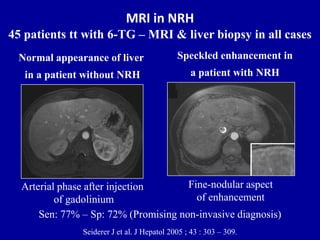
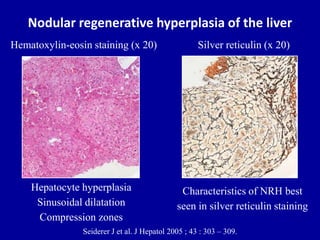
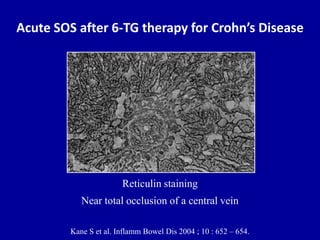
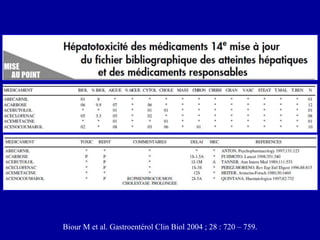
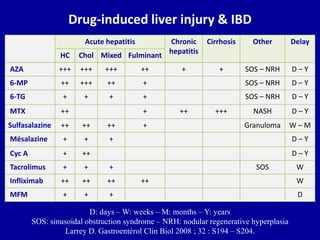
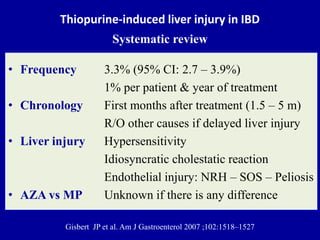
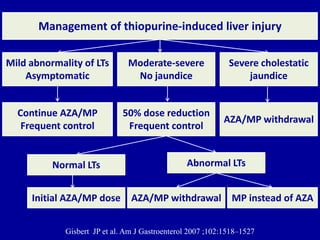
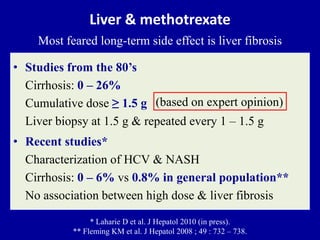
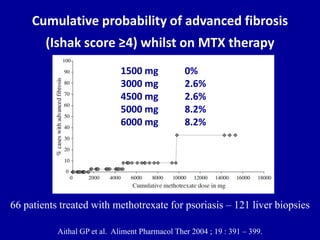
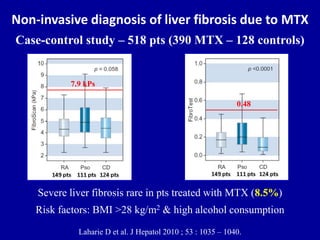
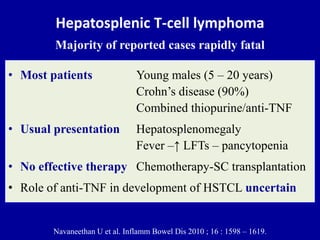
3) Several liver conditions have been reported in association with IBD or its treatments, including gallbladder disease, vascular diseases, nodular regenerative hyperplasia, and drug-induced hepatotoxicity from medications like azathioprine.