Downloaded 257 times






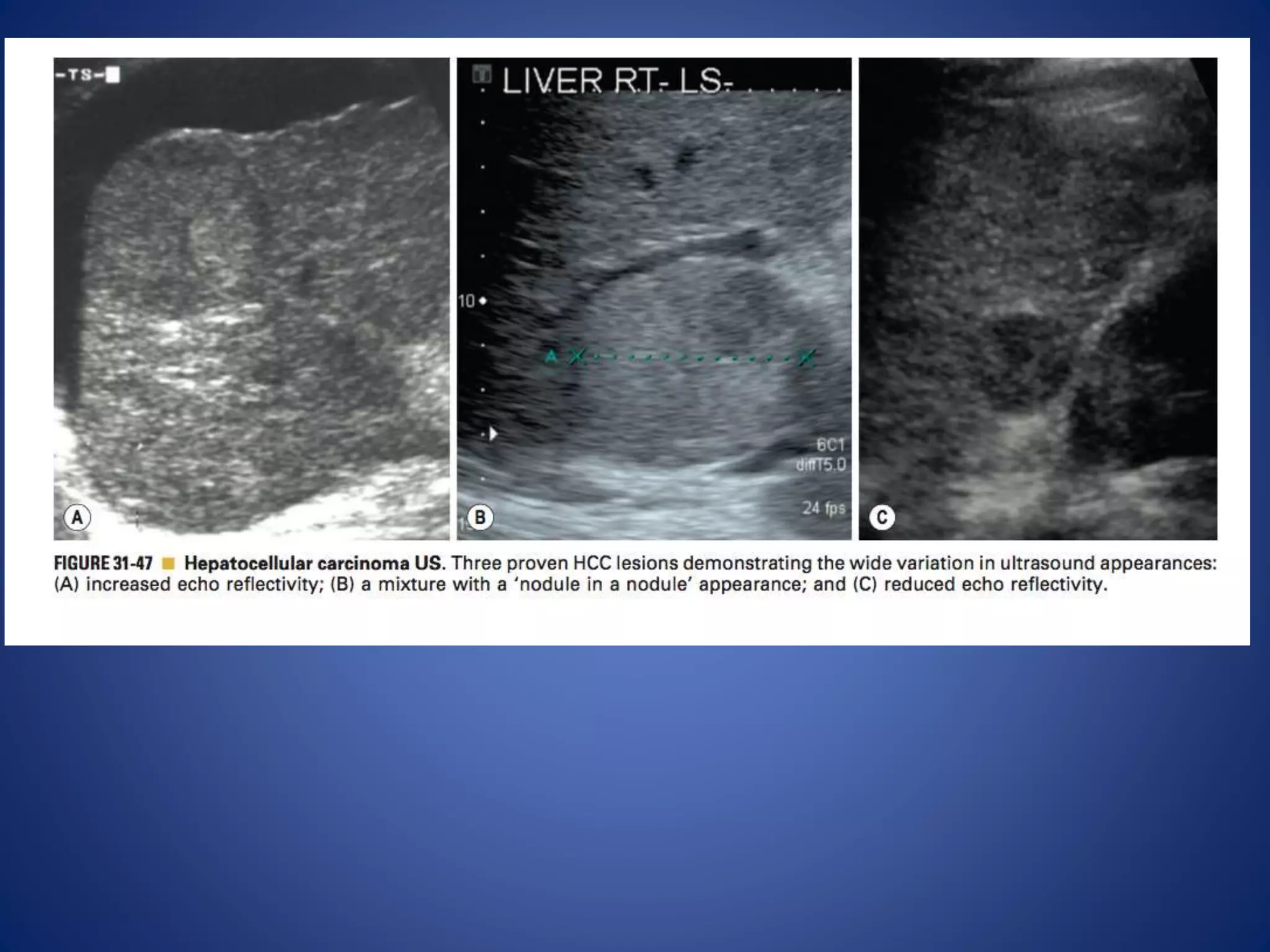






















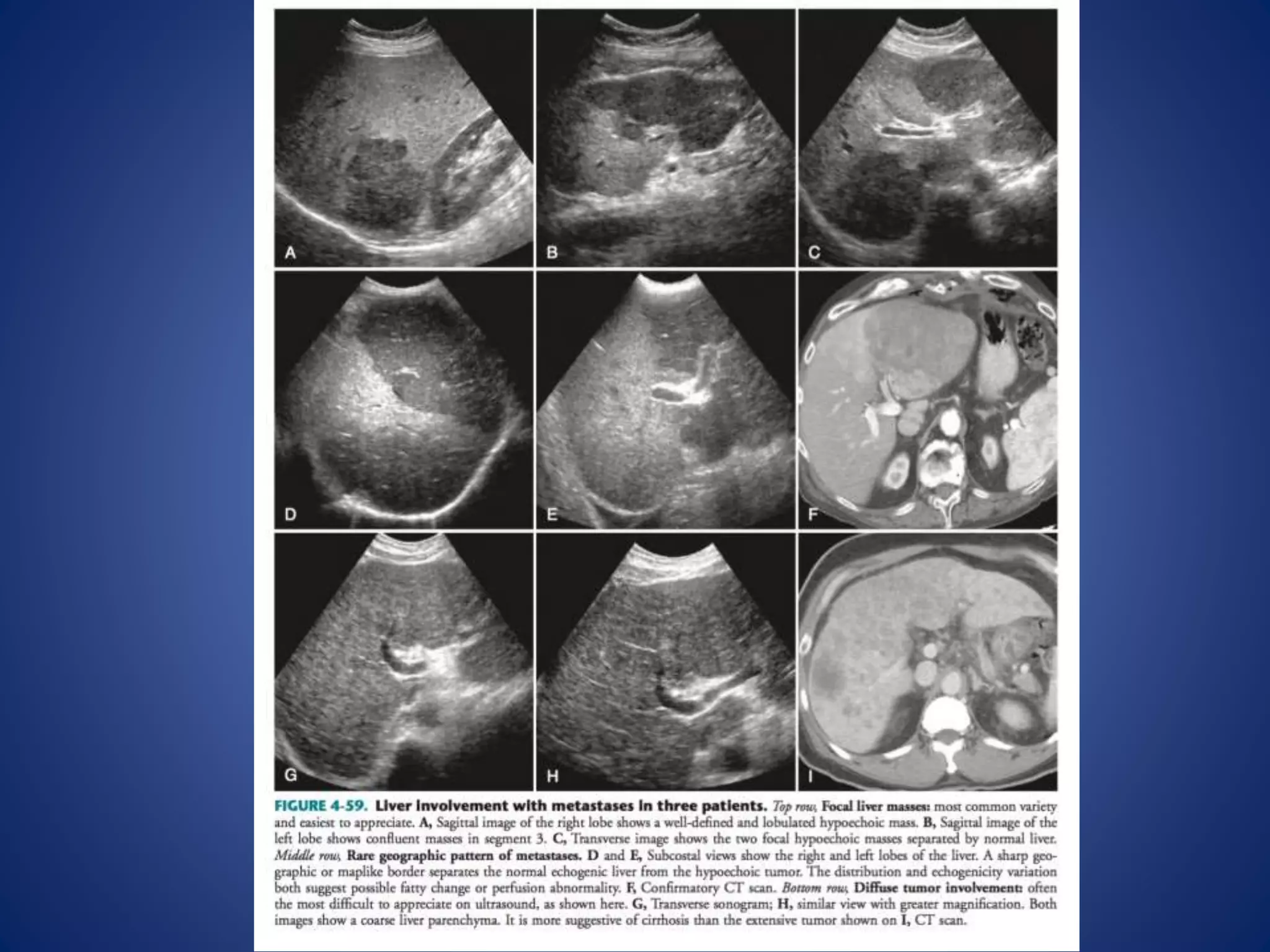



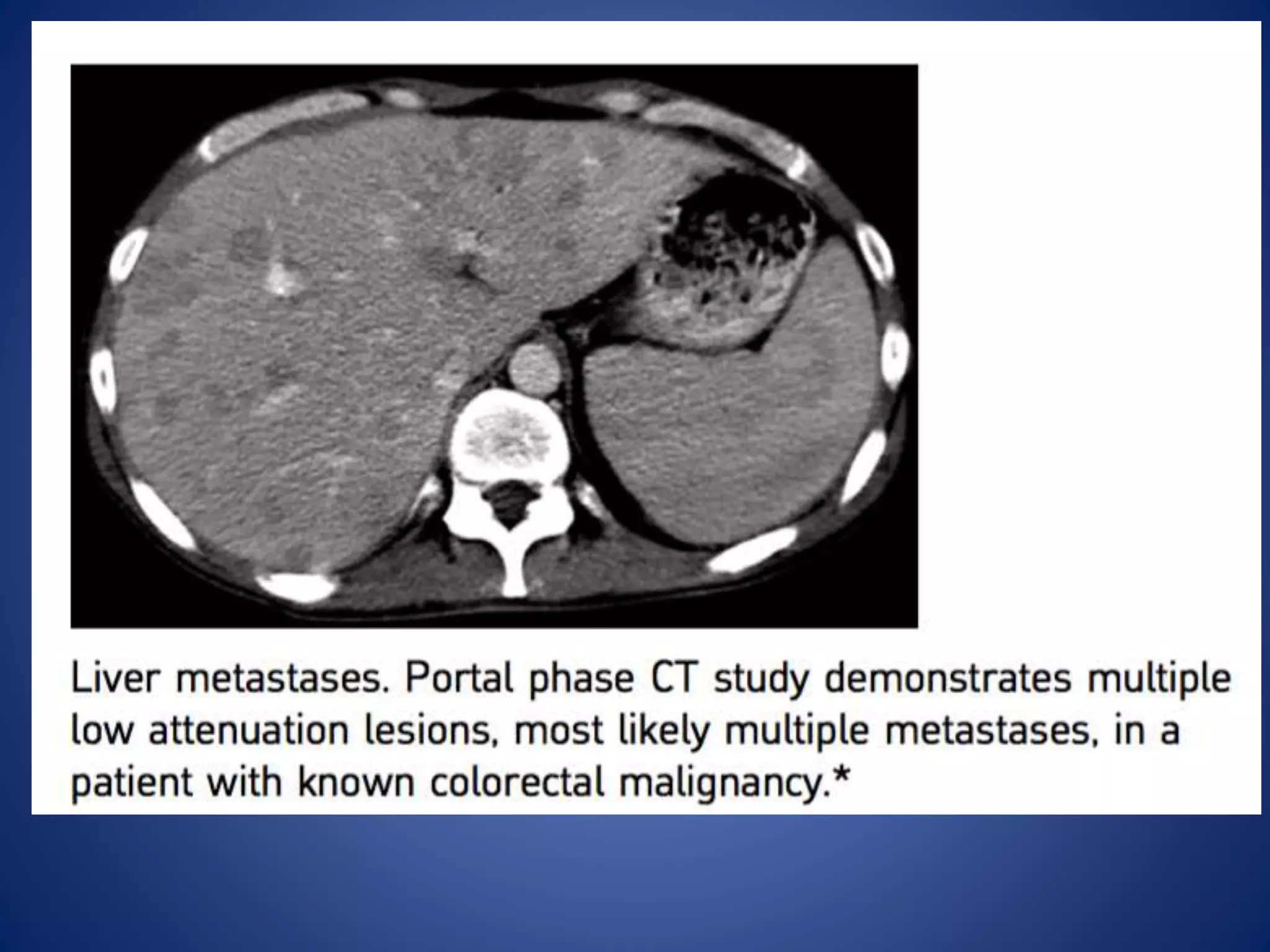



















This document discusses various malignant liver lesions including hepatocellular carcinoma (HCC), liver metastases, and angiosarcoma. HCC is the most common primary liver cancer, often occurring in cirrhotic livers, and can appear solitary or multifocal on imaging. Liver metastases commonly spread from gastrointestinal or non-gastrointestinal primary cancers via the hepatic artery or portal vein. Angiosarcoma is a rare malignant vascular liver tumor associated with toxins like polyvinylchloride and arsenic.























































































