Downloaded 1,858 times
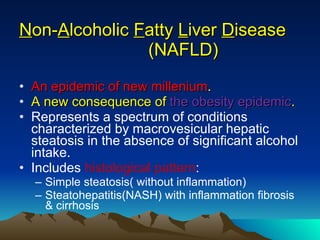
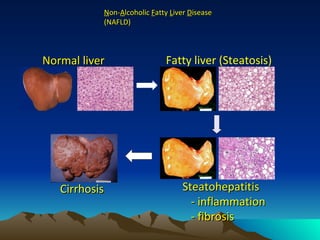


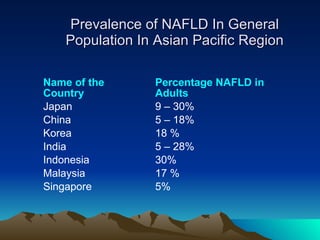
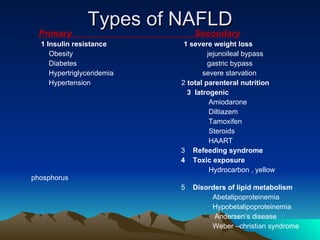
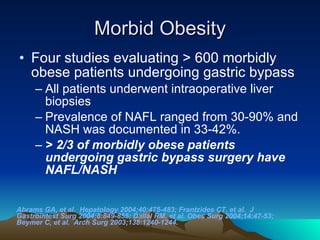
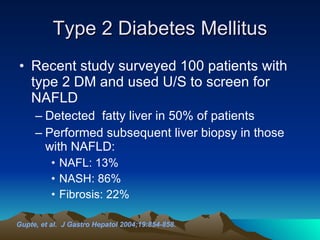
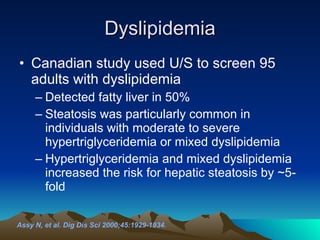
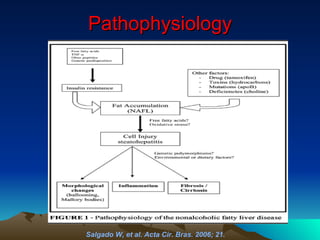
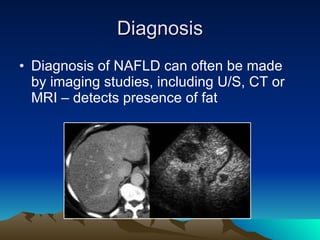
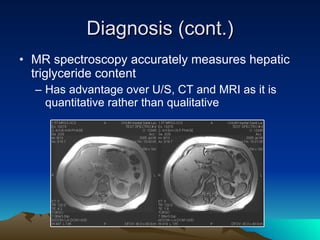


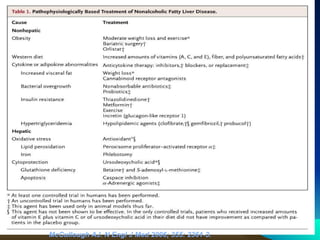

The document discusses non-alcoholic fatty liver disease (NAFLD), which includes a spectrum of conditions from simple steatosis to non-alcoholic steatohepatitis (NASH) and cirrhosis. NAFLD is strongly associated with obesity and metabolic syndrome. The prevalence of NAFLD is increasing globally and varies from 5-30% in different regions. Diagnosis requires imaging and liver biopsy. Treatment focuses on lifestyle modifications and medications to improve insulin resistance.























![Fatty liver disease with Diabetes Mellitus [BANGLADESH]](https://cdn.slidesharecdn.com/ss_thumbnails/fattyliverwithdmfinal-160520141759-thumbnail.jpg?width=640&height=640&fit=bounds)











































