High resolution manometry (HRM) is the most accurate non-invasive test for diagnosing sliding hiatal hernia. HRM can classify hiatal hernias as no hernia, small (1-2 cm separation), or large (>2 cm separation) based on the distance between the lower esophageal sphincter and crural diaphragm pressure zones. A study found HRM had 94% sensitivity and 91% specificity for diagnosing hiatal hernia compared to open surgical assessment, outperforming barium swallow radiography and upper endoscopy. HRM is concluded to be the best test for accurately diagnosing and classifying the size of sliding hiatal hernias.
various congenital gastrointestinal diseases manifesting in childhood or even in adults, their radiographic findings on various imaging modalities such as radiograph, barium, ultrasound etc.
International Journal of Pharmaceutical Science Invention (IJPSI) is an international journal intended for professionals and researchers in all fields of Pahrmaceutical Science. IJPSI publishes research articles and reviews within the whole field Pharmacy and Pharmaceutical Science, new teaching methods, assessment, validation and the impact of new technologies and it will continue to provide information on the latest trends and developments in this ever-expanding subject. The publications of papers are selected through double peer reviewed to ensure originality, relevance, and readability. The articles published in our journal can be accessed online.
Basic of Small Animals Stomach Surgery
Grossly, the stomach is divided into the cardia, fundus, body, and pyloric portions. The point where the intraabdominal esophagus blends into the stomach on the left side is termed the cardia. The cardiac notch is formed between the cardia and the blind outpouching of the stomach, termed the fundus. On the medial aspect the esophagus joins the lesser curvature of the stomach without a distinct anatomic landmark of the junction. The incisura angularis (angular notch) produces an intraluminal protrusion of tissue at approximately the midpoint of the lesser curvature that separates the antrum and the body. This angular notch is the area in which the papillary process of the liver lies......
By DR.Kambiz Yousefi
Kambiz.u3fi@me.com
Drs. Penzler, Ricker, and Ahmad’s CMC Abdominal Imaging Mastery Project: Dece...Sean M. Fox
Dr. Morgan Penzler is an Emergency Medicine Resident and Drs. Raza Ahmad and Ansley Ricker are Surgery Residents at Carolinas Medical Center in Charlotte, NC. They are interested in medical education. With the guidance of Drs. Kyle Cunningham and Michael Gibbs, they aim to help augment our understanding of emergent abdominal imaging. Follow along with the EMGuideWire.com team as they post these monthly educational, self-guided radiology slides. This month’s cases include:
- Gastric Perforation
- Pneumoperitoneum
- Lower GI Bleed
- Parastomal Hernia
Abstract
This case report describes the diagnosis and management of a large mesenteric cyst in a 55 year old lady who presented with abdominal distension & with mass in the left upper quadrant. Mesenteric cysts are rare, benign, abdominal tumors to which <1000 cases have been reported in the literature. While 40% of cases are incidental findings found either through physical examination or imaging, they can cause non-specific abdominal symptoms including pain, altered bowel habits, nausea/vomiting or anorexia. Less commonly, 10% of cases can present with bowel obstruction, volvulus, torsion or shock. In general, the lack of characteristic clinical and radiological features presents as a diagnostic difficulty.
The mainstay in imaging is computerized tomography (CT). CT identifies and helps aid the decision to pursue a laparoscopic or open laparotomy approach, where complete surgical resection is the ultimate goal. In our patient a CT Abdomen & Pelvis showed a large, loculated cystic mass measuring 30cm in cranio-caudal length and 16cm in the transverse and anterior/posterior diameter. While different approaches have been described in the literature to surgically resect such cysts, our approach was largely reflective of size and adherence to surrounding structures in this case. A laparotomy was performed using an upper mid-line 7 cm incision; 4500cc of fluid was aspirated from the cyst which was found to originate from the small bowel mesentery. A complete resection of the multi-loculated cystic sac was done that included the resection of the middle mesenteric vein. The post-operative period was uneventful. The patient was discharged on post-operative day 2. The Histopathology identified the mass as a multi-loculated peritoneal inclusion-type cyst.
Drs. Lena, Avery, and Davis’s CMC Abdominal Imaging Mastery Project: October ...Sean M. Fox
Dr. Kelsey Lena is an Emergency Medicine Resident and Drs. Michael Avery and Joshua Davis are Surgery Residents at Carolinas Medical Center in Charlotte, NC. They are interested in medical education. With the guidance of Drs. Kyle Cunningham and Michael Gibbs, they aim to help augment our understanding of emergent abdominal imaging. Follow along with the EMGuideWire.com team as they post these monthly educational, self-guided radiology slides. This month’s topics include:
• Perforated gastric ulcer
• May Thurner Syndrome
• Hematocolpos
Similar to Diagnosis of sliding hiatal hernia (20)
Description of various ultrasound features of benign and suspicious thyroid nodules with multiple ultrasound systems for risk stratification of malignancy.
Description of different ultrasound features of carpal tunnel syndrome before and after carpal tunnel release including Doppler imaging and elastography
Doppler ultrasound of visceral arteriesSamir Haffar
Doppler ultrasound of different diseases of visceral arteries including arterial stenosis and occlusion, arterial aneurysm, artrial pseudoaneurysm, arterio-venous fistula, artrial dissection, and abdominal vascular compression syndromes
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
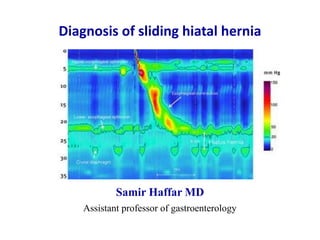
1. Diagnosis of sliding hiatal hernia
Samir Haffar MD
Assistant professor of gastroenterology
2. Diagnosis of sliding hiatal hernia
① Types of hiatal hernia
② Barium swallow radiography
③ Upper gastrointestinal endoscopy
④ Standard esophageal manometry
⑤ High resolution manometry (HRM)
4. Type of hiatal hernia
Normal anatomy Type I Type II Type III
sliding hiatal hernia paraesophageal hernia mixed hiatal hernia
most common (95%)
Duranceau A. Dis Esophagus 2016;29(4):350–66.
5. Normal anatomy
Ishimura N et al. Dig Endoscopy 2009;21:213–218.
Distance between squamous-columnar junction
and diaphragmatic indentation < 2 cm
6. Hiatal hernia type 1
sliding hiatal hernia
most common form (95%)
Duranceau A. Dis Esophagus 2016;29(4):350–66.
Distance between squamous-columnar junction
and diaphragmatic indentation > 2 cm
7. Endoscope emerges from gastroesophageal junction
which is in normal position
The endoscope retroflexes and looks at stomach fundus
herniated through diaphragm
Duranceau A. Dis Esophagus 2016;29(4):350–66.
Hiatal hernia type 2
para-esophageal hiatal hernia
8. Duranceau A. Dis Esophagus 2016;29(4):350–66.
Forward view of massive herniation observed from
gastroesophageal junction at 30 cm from incisors
Retroflexed view under the diaphragm of a type III hernia
and an enlarged hiatus
Hiatal hernia type 3
mixed hiatal hernia
Forward view Retroflexed view
10. Kahrilas PJ et al. Best Practice Research Clin Gastroenterol 2008;22(4):601–616.
Anatomical features of sliding hiatal hernia
viewed radiographically
Ring A: Superior margin of LES (highest pressure zone in LES)
Ring B: At squamocolumnar junction, present in 15% of persons
Division of phrenic ampulla into oesophageal vestibule (A
to B ring) & HH (B ring to sub-diaphragmatic stomach)
Hiatal hernia: Distance from B ring to hiatus > 2 cm
11. Barium swallow radiography
Kahrilas PJ et al. Best Practice Research Clin Gastroenterol 2008;22(4):601–616.
Well developed ring A and ring B
Hiatal hernia defined by distance from B ring to hiatus > 2 cm
Image in early swallow: hiatus hernia indicated by black bracket
Image in late swallow: hiatus hernia indicated by white bracket
Size estimate of hiatal hernia depends on when in the swallow
sequence the measurement is made
Early swallow Late swallow
12. Limitations of barium swallow radiography
• Not all of previous structures always demonstrable radiographically
• Commonly, A ring but not B ring is evident and thus the limits
of measurement defining hiatus hernia become arbitrary
• B ring located at SCJ only demonstrable in only 15% of individuals
• Measurement of B ring to hiatus depends on timing of swallow:
early swallow, late swallow or between swallows
• Frequency of sliding hiatus hernia increased in case of abdominal
compression during barium swallow imaging
Prevalence of sliding hiatal hernia vary enormously from 10 – 80%
Identification of type 1 hernia < 3 cm by radiography is unreliable
Kahrilas PJ et al. Best Practice Research Clin Gastroenterol 2008;22(4):601–616.
13. Hyun JJ et al. Gut and Liver 2011;5(3):267–277.
Barium swallow radiography
When sliding hiatal hernia is > 3 cm, is its
presence obvious because gastric folds are
evident traversing diaphragm both during
swallow-induced shortening & at rest
diaphragmatic
indentation
diaphragmatic
indentation
15. Upper gastrointestinal endoscopy
forward view
Sliding hiatus hernia diagnosed when
distance between squamocolumnar junction
and diaphragmatic impression > 2 cm
Accuracy and reproducibility of such
measurements have not been tested
Kahrilas PJ et al. Best Practice Research Clin Gastroenterol 2008;22(4):601–616.
16. Kahrilas PJ et al. Best Practice Research Clin Gastroenterol 2008;22(4):601–616.
Gastro-esophageal area open all the time
Squamous epithelium of distal esophagus seen from retroflexed view
Sliding hiatal hernia is always present with this deformity
Upper gastrointestinal endoscopy
retroflexed view
17. Limitations of upper gastrointestinal endoscopy
• Extremely patulous hiatus:
Difficulty to precisely localize the crural diaphragm
• Excess insufflation of stomach
Might exaggerate the apparent size of hernia
• Barrett’s metaplasia:
Difficulty to ascertain location of native squamocolumnar junction
HH: hiatal hernia
Kahrilas PJ et al. Best Practice Research Clin Gastroenterol 2008;22(4):601–616.
Little study of sensitivity of endoscopic measurement of sliding HH
Endoscopy suffers from similar limitations to barium swallow
Identification of type I hernia < 3 cm with endoscopy is unreliable
19. Standard esophageal manometry in hiatal hernia
one circumferential sensor distally & pulled out by 0.5 cm steps
Fornari F et al. Dig Liver Dis 2009;41:886–890.
Dual high-pressure zones at gastro-esophageal junction
Distal hump corresponds to diaphragmatic crura
Proximal hump corresponds to lower esophageal sphincter
20. Fornari F et al. Dig Liver Dis 2009;41:886–890.
Diagnostic accuracy of conventional manometry
Endoscopy as the referential technique
Percentage 95% confidence interval
Sensibility 28% 19 – 40
Specificity 97% 93 – 99
Positive predictive value 82% 63 – 92
Negative predictive value 76% 73 – 79
Study of 215 consecutive patients with or without HH
22. Normal HRM following a wet swallow
EGJ: esophago-gastric junction – LES: lower esophageal junction
Conklin JL. J Neurogastroenterol Motil 2013;19(3):281–294.
UES: Upper esophageal sphincter
S1: Striated esophageal muscle
TZ: Transition zone from striated to smooth muscle
S2: Proximal esophageal smooth muscle
S3: Distal esophageal smooth muscle
S4: LES repositioning itself at its resting position
EGJ: Esophago-gastric junction
Composed of tonic LES contraction & phasic
crural diaphragm contraction with inspiration
23. • Thoracic cavity: Pressure decreases during inspiration
Pressure increases during expiration
• Abdominal cavity: Pressure increases during inspiration
Pressure decreases during expiration
• Pressure inversion point: Point at which pressure across EGJ during
“PIP” inspiration becomes negative
Indicates location of crural diaphragm
Esophago-gastric junction
Composed of tonic LES contraction and cyclic crural contraction
Conklin JL. J Neurogastroenterol Motil 2013;19(3):281–294.
24. Esophago-gastric junction in HRM
• Type I: no separation between LES & CD (normal)
• Type II: 1 – 2 cm separation (small hiatal hernia)
• Type III: > 2 cm of separation (large hiatal hernia)
Distance between maximal LES pressure & maximal CD pressure
CD: crural diaphragm – HRM: high resolution manometry – LES: lower esophageal sphincter
Tolone S et al. United Eur Gastroenterol J 2018;6(7)981–989.
25. Esophago-gastric junction type I
E: expiration – EGJ: esophago-gastric junction – I: inspiration – LES: lower esophageal junction
Conklin JL. J Neurogastroenterol Motil 2013;19(3):281–294.
** tonic LES contraction
* cyclic crural contraction with respiration
red arrowhead: location of pressure inversion point (PIP)
EGJ type 1: normal
coincident LES and crural diaphragm
distancefromnares(cm)
I E
26. Esophago-gastric junction type II
E: expiration – EGJ: esophago-gastric junction – I: inspiration – LES: lower esophageal junction
Conklin JL. J Neurogastroenterol Motil 2013;19(3):281–294.
** tonic LES contraction
* cyclic crural contraction with respiration
red arrowhead: location of pressure inversion point (PIP)
EGJ type 2: small sliding hiatal hernia
LES-crural diaphragm separation 1-2 cm
distancefromnares(cm)
27. E: expiration – EGJ: esophago-gastric junction – I: inspiration – LES: lower esophageal junction
Conklin JL. J Neurogastroenterol Motil 2013;19(3):281–294.
Esophago-gastric junction type III
** tonic LES contraction
* cyclic crural contraction with respiration
red arrowhead: location of pressure inversion point (PIP)
EGJ type 3: large sliding hiatal hernia
LES-crural diaphragm separation > 2 cm
distancefromnares(cm)
I E
28. Types of esophageal-gastric junction
Distance between maximal LES pressure & maximal CD pressure
CD: crural diaphragm – HRM: high resolution manometry – LES: lower esophageal sphincter
Tolone S et al. United Eur Gastroenterol J 2018;6(7)981–989.
Type I Type II Type III
Coincident LES & CD
normal
1 – 2 cm separation
small hiatal hernia
> 2 cm separation
large hiatal hernia
29. Large sliding hiatal hernia
Three high pressure zones: UES, LES and crural diaphragm
Swallow followed by propagated contraction along esophagus
LES & crural diaphragm separated by more than 2 cm
LES: lower esophageal sphincter – UES: upper esophageal sphincter
Roman S et al. BMJ 2014;349:g6154.
30. Diagnostic accuracy of radiography, endoscopy and HRM
Open surgical assessment as gold standard
AUROC: area under receiver operating characteristic – HRM : high resolution manometry
Tolone S et al. United Eur Gastroenterol J 2018;6(7)981–989.
Study of 100 consecutive patients
Radiography Gastroscopy HRM
Sensibility 70% 96% 94%
Specificity 98% 74% 91%
Positive predictive value 97% 81% 93%
Negative predictive value 74% 95% 93%
Kappa value 0.66 0.72 0.85
AUROC – – 0.929
31. Conclusion
• HRM can accurately diagnose sliding hiatal hernia with
high sensibility and specificity
• HRM seems to classify sliding hiatal hernia (no hiatal hernia,
small or large size) better than radiography and endoscopy
• HRM reaches optimal agreement w open surgical assessment
HRM: high resolution manometry