Downloaded 194 times
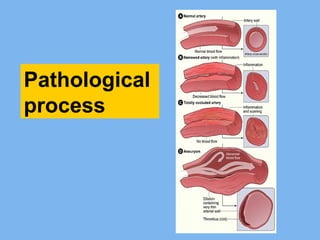
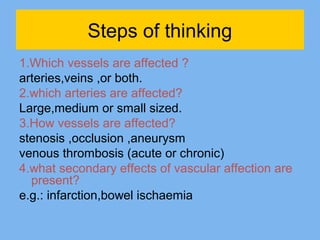
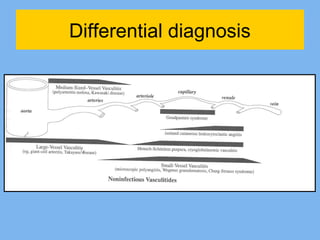
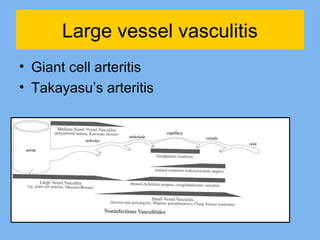
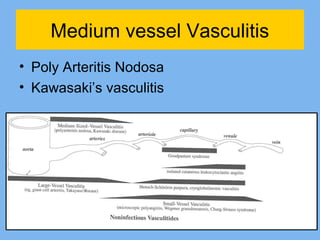
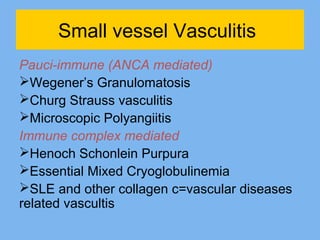
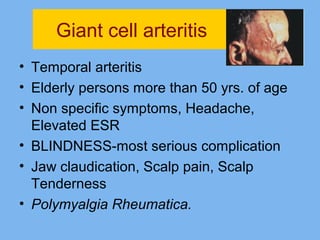
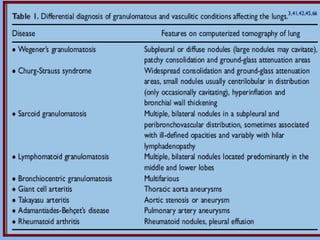
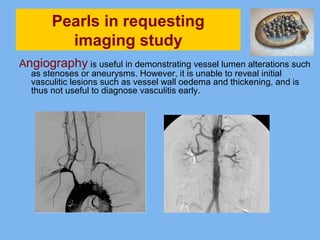
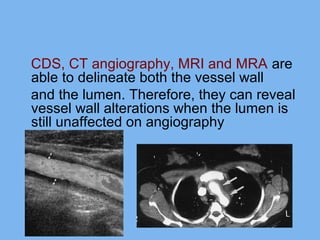
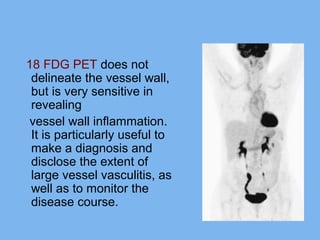


Vasculitis is a condition characterized by inflammation and damage to blood vessels. There are several types of vasculitis classified by the size of vessels affected (large, medium, small). Imaging plays an important role in the diagnosis and monitoring of vasculitis by detecting vessel wall abnormalities and inflammation before lumen changes occur on angiography. Techniques like CT angiography, MRI, MRA, and PET are useful for revealing vessel wall alterations and inflammation. The choice of imaging depends on the suspected organ involvement.





























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













