Downloaded 32 times




![
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1798473/
http://www.medscape.com/viewarticle/407580_1
http://emedicine.medscape.com/article/329255-overview
http://link.springer.com/article/10.1186/2110-5820-2-31
http://www.emdocs.net/the-emergency-medicine-approach-to-vasculitides/
https://emergency.unboundmedicine.com/emergency/view/5-
Minute_Emergency_Consult/307249/all/Vasculitis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4029362/
http://emedicine.medscape.com/article/332483-treatment
http://www.medscape.com/viewarticle/740972_8
http://ard.bmj.com/content/64/5/784
Kawasaki T. [Acute febrile mucocutaneous syndrome with lymphoid
involvement with specific desquamation of the fingers and toes in children].
Arerugi. 1967 Mar. 16(3):178-222. [Medline].
References](https://image.slidesharecdn.com/vasculitisjoshuaho-170518025447/85/Vasculitides-Emergency-Presentations-42-320.jpg)

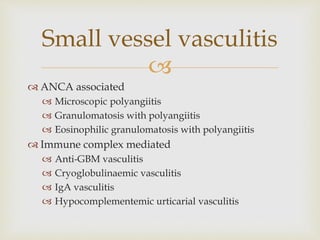
Dr Joshua Ho presented on vasculitis at an emergency medicine CME. Vasculitis refers to inflammation of blood vessels and can affect vessels of any size. The presentation discussed the definitions, pathophysiology involving immune complexes and antibodies, Chapel Hill classification system of different types, common organ systems involved, and emergency presentations such as diffuse alveolar hemorrhage or cerebral vasculitis. Management in the emergency department focuses on recognizing red flags and treating life-threatening manifestations while working up the underlying diagnosis.























































































