Downloaded 158 times
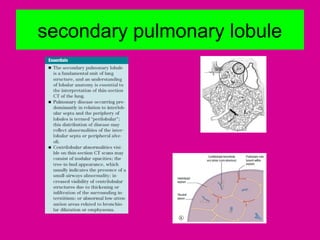
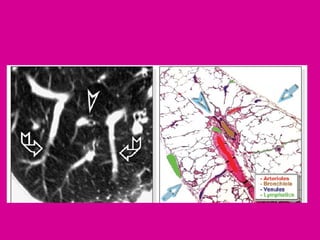
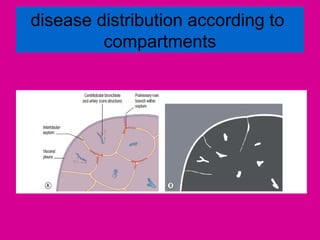
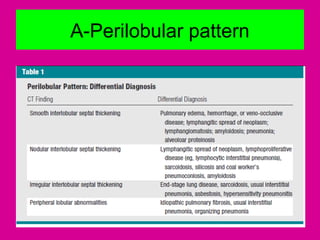
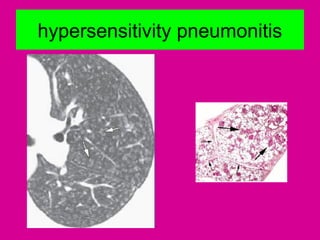
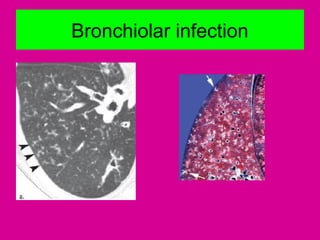
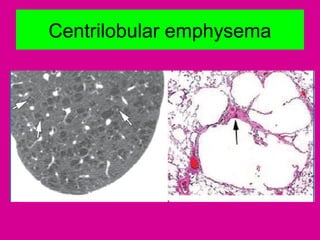
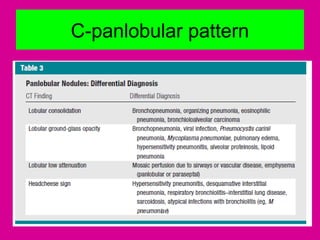
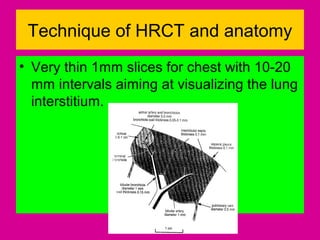
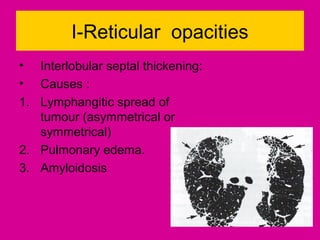
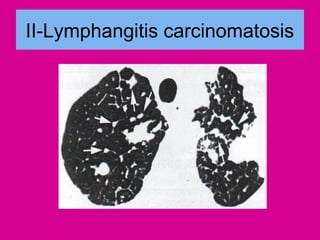
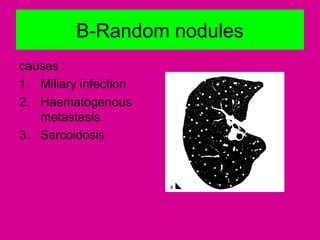
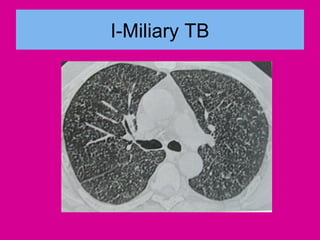
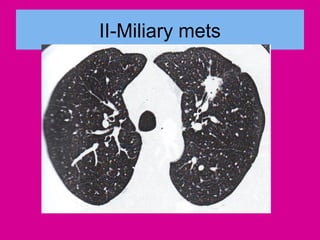
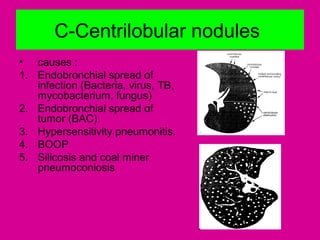
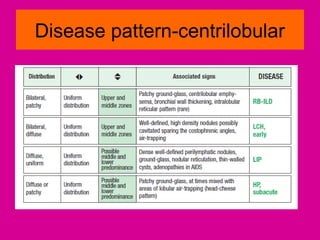
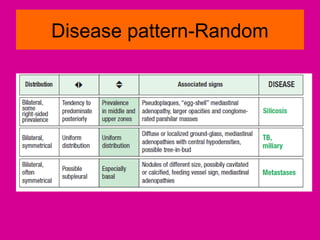
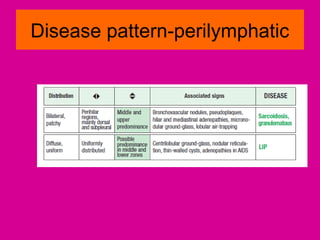
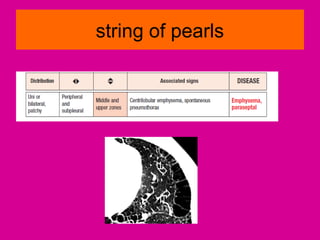
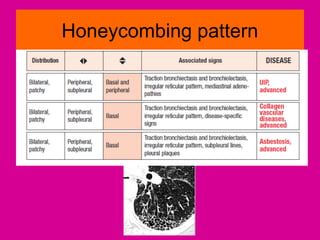
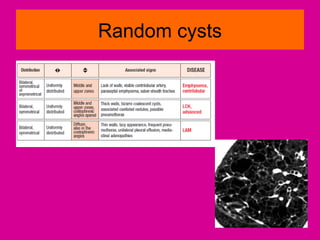
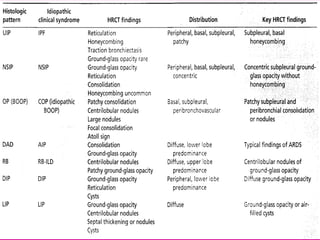
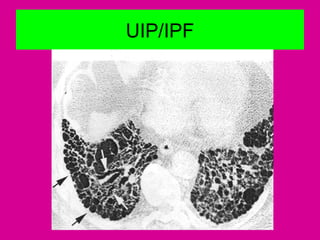
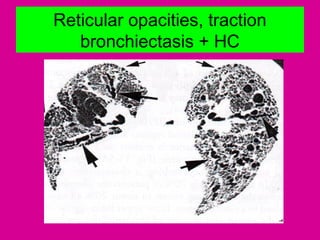
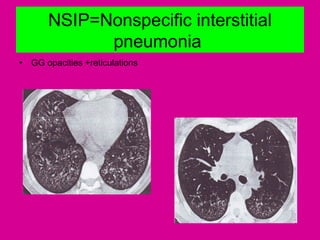
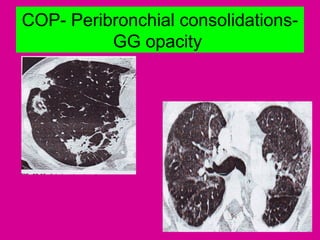
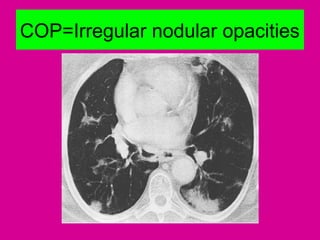
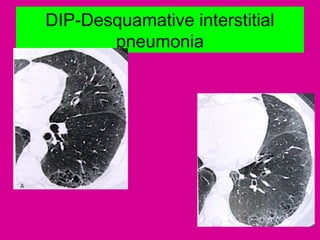
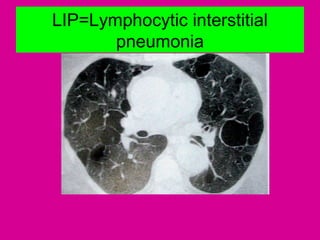
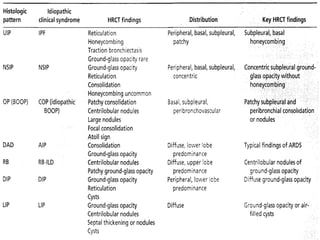
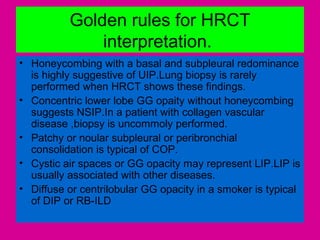


This document discusses how to report findings from HRCT scans of the lungs in patients with interstitial lung disease. It begins by describing the scanning technique and basic lung anatomy. It then outlines a systematic approach to interpretation, including recognizing patterns (reticular, nodular, increased/decreased opacity), locating abnormalities, and evaluating effects on lung parenchyma. Specific disease patterns and findings are discussed along with their typical causes. Golden rules for interpretation are provided. References for further reading are included.